

Primary treatment of acromegaly with high-dose lanreotide: a case series
- PMID: 20211008
- PMCID: PMC2845144
- DOI: 10.1186/1752-1947-4-85
Primary treatment of acromegaly with high-dose lanreotide: a case series
Abstract
Introduction: The first-line treatment for acromegaly is transsphenoidal surgery. In approximately 50% of patients, however, a cure is not possible with surgery and alternatives are needed. Somatostatin analog therapy is the recommended first-line treatment in patients with such cases. Here we provide the first report of a high-dose lanreotide primary therapy in patients with acromegaly.
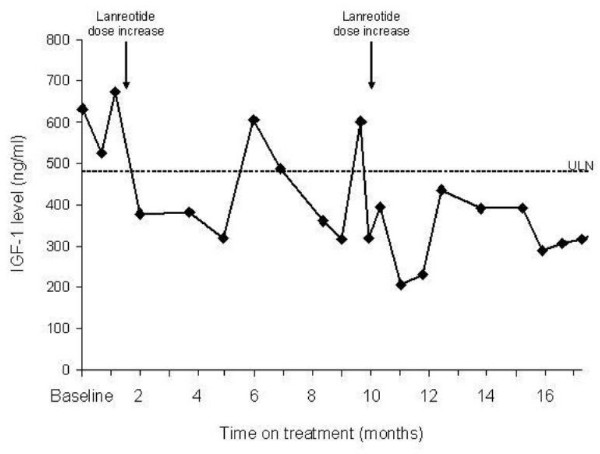
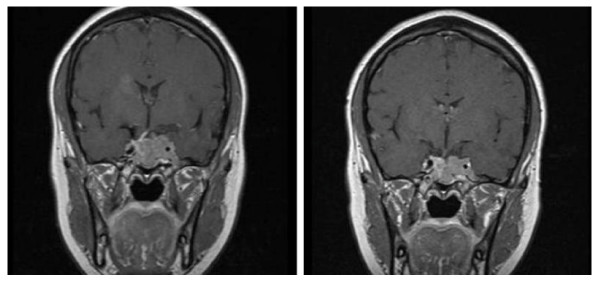
Case presentation: Six patients who were not suitable for surgery were given 60 mg of lanreotide (Autogel(R)) every four weeks. All patients were German nationals and Caucasian.When the response of our patients was unsatisfactory, the dose was increased sequentially to 90 mg every four weeks, 120 mg every four weeks, 120 mg every three weeks and 180 mg every three weeks. Treatment duration was 12 to 24 months. In all cases, the lanreotide dose was 120 mg every 4 weeks or higher. In five of our patients, growth hormone (GH) levels were successfully reduced (in three patients GH <2.5 ng/ml was achieved). Insulin-like growth factor 1 levels were normalized in three patients and decreased in two patients. One patient failed to show a biochemical response to lanreotide therapy or pegvisomant therapy.Tumor shrinkage or degeneration was observed in the five responding patients. No drug-related adverse events were noted.
Conclusions: These results suggest that lanreotide at high doses of 120 mg every four weeks or more is an effective first-line therapy for patients with acromegaly that surgery alone cannot treat.
Figures
Similar articles
-
Pegvisomant: new preparation. A last resort in acromegaly.Prescrire Int. 2005 Feb;14(75):10-3. Prescrire Int. 2005. PMID: 15751152
-
Systematic dose-extension of octreotide LAR: the importance of individual tailoring of treatment in patients with acromegaly.Clin Endocrinol (Oxf). 2004 Aug;61(2):224-31. doi: 10.1111/j.1365-2265.2004.02084.x. Clin Endocrinol (Oxf). 2004. PMID: 15272918
-
Therapeutic options in the management of acromegaly: focus on lanreotide Autogel.Biologics. 2008 Sep;2(3):463-79. doi: 10.2147/btt.s3356. Biologics. 2008. PMID: 19707377 Free PMC article.
-
The role of lanreotide Autogel® in the treatment of acromegaly.Expert Rev Endocrinol Metab. 2007 Jul;2(4):433-441. doi: 10.1586/17446651.2.4.433. Expert Rev Endocrinol Metab. 2007. PMID: 30290426
-
Severe scalp hair loss in a female patient with acromegaly treated with lanreotide autogel after unsuccessful surgery.Clin Case Rep. 2015 Nov;3(11):945-8. doi: 10.1002/ccr3.388. Epub 2015 Oct 7. Clin Case Rep. 2015. PMID: 26576278 Free PMC article.
Cited by
-
Clinical efficacy and safety results for dose escalation of somatostatin receptor ligands in patients with acromegaly: a literature review.Pituitary. 2011 Jun;14(2):184-93. doi: 10.1007/s11102-010-0282-z. Pituitary. 2011. PMID: 21161602 Free PMC article. Review.
-
Management options for persistent postoperative acromegaly.Neurosurg Clin N Am. 2012 Oct;23(4):621-38. doi: 10.1016/j.nec.2012.06.005. Epub 2012 Aug 9. Neurosurg Clin N Am. 2012. PMID: 23040748 Free PMC article. Review.
-
The treatment of neuroendocrine tumors with long-acting somatostatin analogs: a single center experience with lanreotide autogel.J Endocrinol Invest. 2011 Oct;34(9):692-7. doi: 10.3275/8058. Epub 2011 Nov 7. J Endocrinol Invest. 2011. PMID: 22067307
References
-
- Kauppinen-Makelin R, Sane T, Reunanen A, Valimaki MJ, Niskanen L, Markkanen H, Loyttyniemi E, Ebeling T, Jaatinen P, Laine H, Nuutila P, Salmela P, Salmi J, Stenman UH, Viikari J, Voutilainen E. A nationwide survey of mortality in acromegaly. J Clin Endocrinol Metab. 2005;90(7):4081–4086. doi: 10.1210/jc.2004-1381. - DOI - PubMed
LinkOut - more resources
Full Text Sources
