

Effect of point-of-care computer reminders on physician behaviour: a systematic review
- PMID: 20212028
- PMCID: PMC2842864
- DOI: 10.1503/cmaj.090578
Effect of point-of-care computer reminders on physician behaviour: a systematic review
Abstract
Background: The opportunity to improve care using computer reminders is one of the main incentives for implementing sophisticated clinical information systems. We conducted a systematic review to quantify the expected magnitude of improvements in processes of care from computer reminders delivered to clinicians during their routine activities.
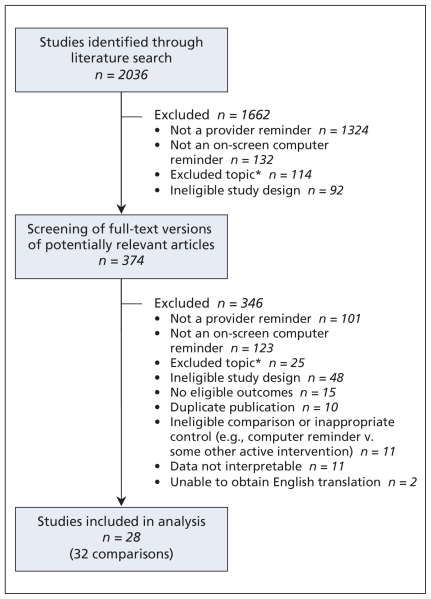
Methods: We searched the MEDLINE, Embase and CINAHL databases (to July 2008) and scanned the bibliographies of retrieved articles. We included studies in our review if they used a randomized or quasi-randomized design to evaluate improvements in processes or outcomes of care from computer reminders delivered to physicians during routine electronic ordering or charting activities.
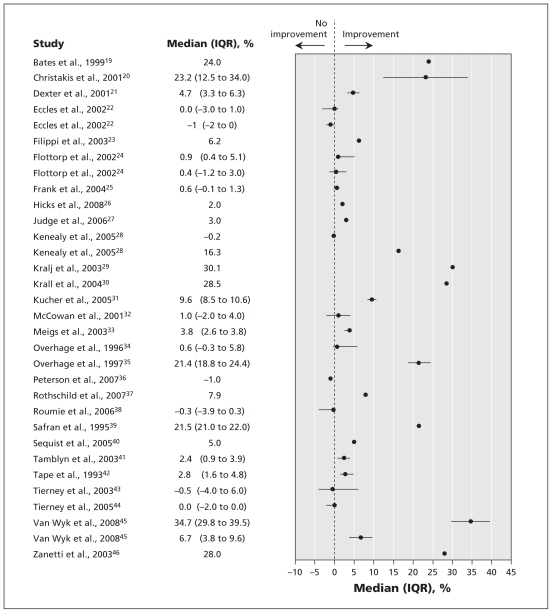
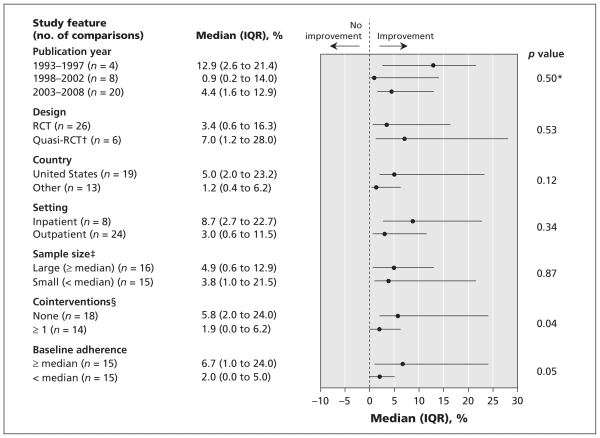
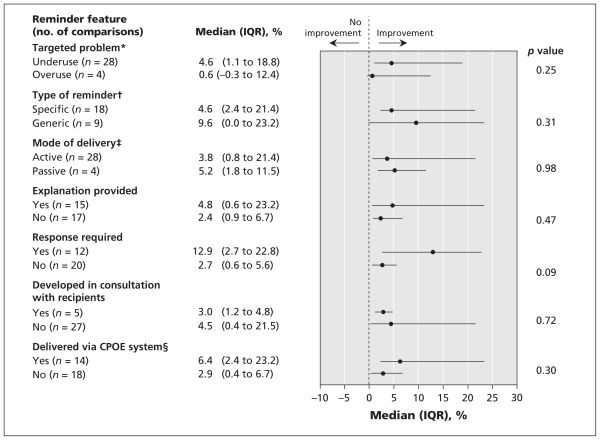
Results: Among the 28 trials (reporting 32 comparisons) included in our study, we found that computer reminders improved adherence to processes of care by a median of 4.2% (interquartile range [IQR] 0.8%-18.8%). Using the best outcome from each study, we found that the median improvement was 5.6% (IQR 2.0%-19.2%). A minority of studies reported larger effects; however, no study characteristic or reminder feature significantly predicted the magnitude of effect except in one institution, where a well-developed, "homegrown" clinical information system achieved larger improvements than in all other studies (median 16.8% [IQR 8.7%-26.0%] v. 3.0% [IQR 0.5%-11.5%]; p = 0.04). A trend toward larger improvements was seen for reminders that required users to enter a response (median 12.9% [IQR 2.7%-22.8%] v. 2.7% [IQR 0.6%-5.6%]; p = 0.09).
Interpretation: Computer reminders produced much smaller improvements than those generally expected from the implementation of computerized order entry and electronic medical record systems. Further research is required to identify features of reminder systems consistently associated with clinically worthwhile improvements.
Figures
Comment in
-
Good prescribing: better systems and prescribers needed.CMAJ. 2010 Apr 6;182(6):540-1. doi: 10.1503/cmaj.100335. Epub 2010 Mar 8. CMAJ. 2010. PMID: 20212024 Free PMC article. No abstract available.
-
Computer reminders to clinicians during routine activities produce only small improvements in adherence to processes of care: median improvement 4.2%, IQR 0.8-18.8%.Evid Based Med. 2010 Aug;15(4):113-4. doi: 10.1136/ebm1081. Epub 2010 Jun 8. Evid Based Med. 2010. PMID: 20530606 No abstract available.
References
-
- Aspden P, Wolcott JA, Bootman JL, et al. Committee on Identifying and Preventing Medication Errors. Preventing medication errors: quality chasm series. Washington (DC): The National Academies Press; 2006.
-
- Garg AX, Adhikari NK, McDonald H, et al. Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review. JAMA. 2005;293:1223–38. - PubMed
-
- Hunt DL, Haynes RB, Hanna SE, et al. Effects of computer-based clinical decision support systems on physician performance and patient outcomes: a systematic review. JAMA. 1998;280:1339–46. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources