

A cluster randomized controlled Trial to Evaluate an Ambulatory primary care Management program for patients with dyslipidemia: the TEAM study
- PMID: 20212029
- PMCID: PMC2842856
- DOI: 10.1503/cmaj.090533
A cluster randomized controlled Trial to Evaluate an Ambulatory primary care Management program for patients with dyslipidemia: the TEAM study
Abstract
Background: Few studies have reported the efficacy of collaborative care involving family physicians and community pharmacists for patients with dyslipidemia.
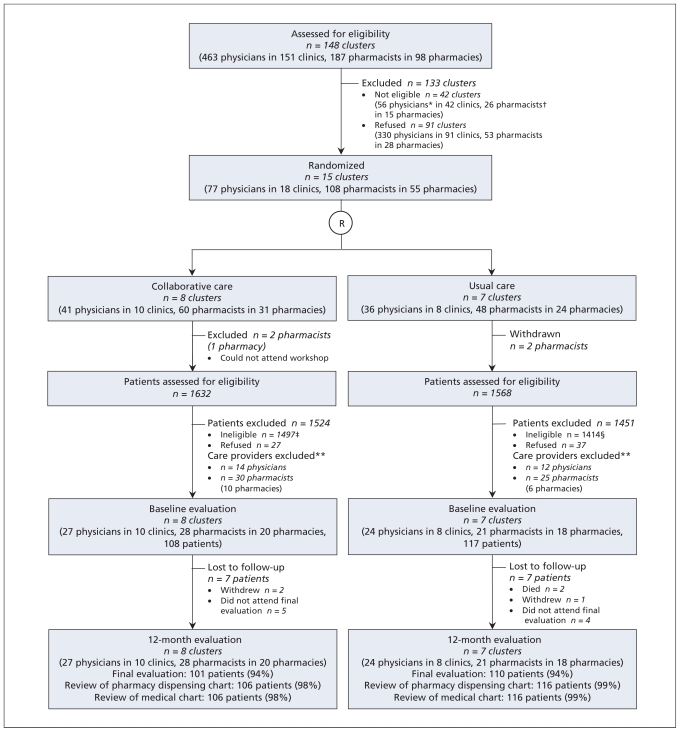
Methods: We randomly assigned clusters consisting of at least two physicians and at least four pharmacists to provide collaborative care or usual care. Under the collaborative care model, pharmacists counselled patients about their medications, requested laboratory tests, monitored the effectiveness and safety of medications and patients' adherence to therapy, and adjusted medication dosages. After 12 months of follow-up, we assessed changes in low-density lipoprotein (LDL) cholesterol (the primary outcome), the proportion of patients reaching their target lipid levels and changes in other risk factors.
Results: Fifteen clusters representing a total of 77 physicians and 108 pharmacists were initially recruited, and a total of 51 physicians and 49 pharmacists were included in the final analyses. The collaborative care teams followed a total of 108 patients, and the usual care teams followed a total of 117 patients. At baseline, mean LDL cholesterol level was higher in the collaborative care group (3.5 v. 3.2 mmol/L, p = 0.05). During the study, patients in the collaborative care group were less likely to receive high-potency statins (11% v. 40%), had more visits with health care professionals and more laboratory tests, were more likely to have their lipid-lowering treatment changed and were more likely to report lifestyle changes. At 12 months, the crude incremental mean reduction in LDL cholesterol in the collaborative care group was -0.2 mmol/L (95% confidence interval [CI] -0.3 to -0.1), and the adjusted reduction was -0.05 (95% CI -0.3 to 0.2). The crude relative risk of achieving lipid targets for patients in the collaborative care group was 1.10 (95% CI 0.95 to 1.26), and the adjusted relative risk was 1.16 (95% CI 1.01 to 1.34).
Interpretation: Collaborative care involving physicians and pharmacists had no significant clinical impact on lipid control in patients with dyslipidemia. International Standard Randomized Controlled Trial register no. ISRCTN66345533.
Figures
Comment in
-
Good prescribing: better systems and prescribers needed.CMAJ. 2010 Apr 6;182(6):540-1. doi: 10.1503/cmaj.100335. Epub 2010 Mar 8. CMAJ. 2010. PMID: 20212024 Free PMC article. No abstract available.
References
-
- Gould AL, Davies GM, Alemao E, et al. Cholesterol reduction yields clinical benefits: meta-analysis including recent trials. Clin Ther. 2007;29:778–94. - PubMed
-
- Avorn J, Monette J, Lacour A, et al. Persistence of use of lipid-lowering medications. A cross-national study. JAMA. 1998;279:1458–62. - PubMed
-
- Bourgault C, Davignon J, Fodor G, et al. Statin therapy in Canadian patients with hypercholesterolemia: the Canadian Lipid Study — Observational (CALIPSO) Can J Cardiol. 2005;21:1187–93. - PubMed
-
- Farahani P, Levine M. Goal attainment for multiple cardiovascular risk factors in community-based clinical practice (a Canadian experience) J Eval Clin Pract. 2009;15:212–6. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical