

Differences in patient survival after acute myocardial infarction by hospital capability of performing percutaneous coronary intervention: implications for regionalization
- PMID: 20212179
- PMCID: PMC2900156
- DOI: 10.1001/archinternmed.2009.538
Differences in patient survival after acute myocardial infarction by hospital capability of performing percutaneous coronary intervention: implications for regionalization
Abstract
Background: There are increasing calls for regionalization of acute myocardial infarction (AMI) care in the United States to hospitals with the capacity to perform percutaneous coronary intervention (PCI). Whether regionalization will improve outcomes depends in part on the magnitude of existing differences in outcomes between PCI and non-PCI hospitals within the same health care region.
Methods: A 100% sample of claims from Medicare fee-for-service beneficiaries 65 years or older hospitalized for AMI between January 1, 2004, and December 31, 2006, was used to calculate hospital-level, 30-day risk-standardized mortality rates (RSMRs). The RSMRs between PCI and local non-PCI hospitals were compared within local health care regions defined by hospital referral regions (HRRs).
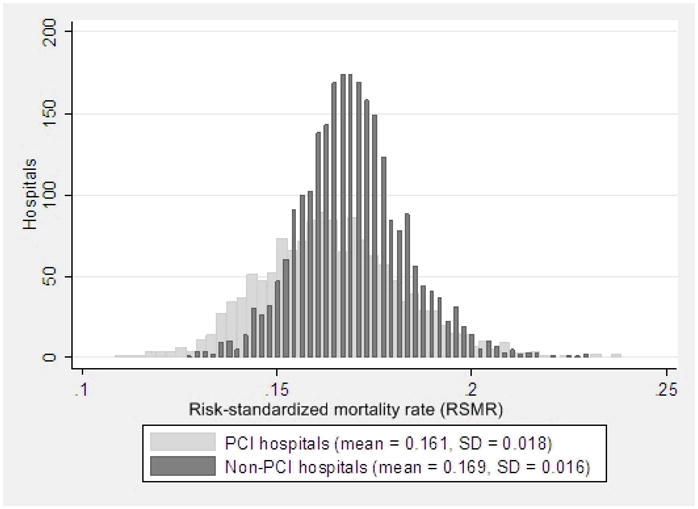
Results: A total of 523 119 AMI patients was admitted to 1382 PCI hospitals, and 194 909 AMI patients were admitted to 2491 non-PCI hospitals in 295 HRRs with at least 1 PCI and 1 non-PCI hospital. Although PCI hospitals had lower RSMRs than non-PCI hospitals (mean, 16.1% vs 16.9%; P < .001), considerable overlap was seen in RSMRs between non-PCI and PCI hospitals within the same HRR. In 80 HRRs, the RSMRs at the best-performing PCI hospital were lower than those at local non-PCI hospitals by 3% or more. Among the remaining HRRs, the RSMRs at the best-performing PCI hospital were lower by 1.5% to 3.0% in 104 HRRs and by greater than 0 to 1.5% in 74 HRRs. In 37 HRRs, the RSMRs at the best-performing PCI hospital were no better or were higher than at local non-PCI hospitals.
Conclusions: The magnitude of benefit from comprehensively regionalizing AMI care to PCI hospitals appears to vary greatly across HRRs. These findings support a tailored regionalization policy that targets areas with the greatest outcome differences between PCI and local non-PCI hospitals.
Conflict of interest statement
The following authors have the potential conflicts of interest to disclose in relation to this study: Dr. Normand is a primary investigator for the Mass-DAC trial examining new capacity of primary PCI centers in Massachusetts. The remaining authors have no conflicts of interest to disclose related to this manuscript.
Figures
References
-
- Califf RM, Faxon DP. Need for centers to care for patients with acute coronary syndromes. Circulation. 2003 Mar 25;107(11):1467–1470. - PubMed
-
- Topol EJ, Kereiakes DJ. Regionalization of care for acute ischemic heart disease: a call for specialized centers. Circulation. 2003 Mar 25;107(11):1463–1466. - PubMed
-
- Andersen HR, Nielsen TT, Rasmussen K, et al. A Comparison of Coronary Angioplasty with Fibrinolytic Therapy in Acute Myocardial Infarction. N Engl J Med. 2003 August 21;349(8):733–742. - PubMed
-
- Grines CL, Westerhausen DR, Jr, Grines LL, et al. A randomized trial of transfer for primary angioplasty versus on-site thrombolysis in patients with high-risk myocardial infarction: the Air Primary Angioplasty in Myocardial Infarction study. J Am Coll Cardiol. 2002 Jun 5;39(11):1713–1719. - PubMed
-
- Widimsky P, Budesinsky T, Vorac D, et al. Long distance transport for primary angioplasty vs immediate thrombolysis in acute myocardial infarction. Final results of the randomized national multicentre trial--PRAGUE-2. Eur Heart J Jan. 2003;24(1):94–104. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
