

Delaying treatment of ocular hypertension: the ocular hypertension treatment study
- PMID: 20212196
- PMCID: PMC3966140
- DOI: 10.1001/archophthalmol.2010.20
Delaying treatment of ocular hypertension: the ocular hypertension treatment study
Abstract
Objective: To compare the safety and efficacy of earlier vs later treatment in preventing primary open-angle glaucoma (POAG) in individuals with ocular hypertension.
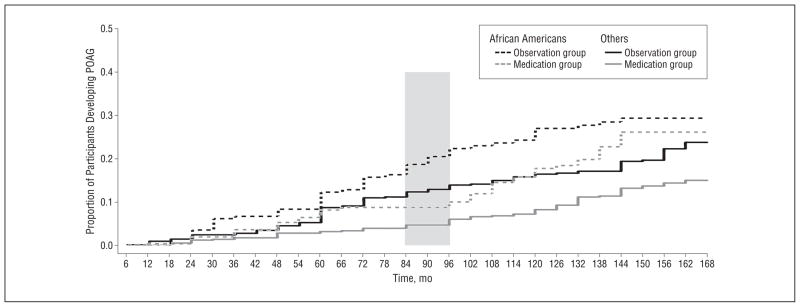
Methods: One thousand six hundred thirty-six individuals with intraocular pressure (IOP) from 24 to 32 mm Hg in 1 eye and 21 to 32 mm Hg in the fellow eye were randomized to observation or to topical ocular hypotensive medication. Median time of treatment in the medication group was 13.0 years. After a median of 7.5 years without treatment, the observation group received medication for a median of 5.5 years. To determine if there is a penalty for delaying treatment, we compared the cumulative proportions of participants who developed POAG at a median follow-up of 13 years in the original observation group and in the original medication group.
Main outcome measures: Cumulative proportion of participants who developed POAG.
Results: The cumulative proportion of participants in the original observation group who developed POAG at 13 years was 0.22 (95% confidence interval [CI], 0.19-0.25), vs 0.16 (95% CI, 0.13-0.19) in the original medication group (P = .009). Among participants at the highest third of baseline risk of developing POAG, the cumulative proportion who developed POAG was 0.40 (95% CI, 0.33-0.46) in the original observation group and 0.28 (95% CI, 0.22-0.34) in the original medication group. There was little evidence of increased adverse events associated with medication.
Application to clinical practice: Absolute reduction was greatest among participants at the highest baseline risk of developing POAG. Individuals at high risk of developing POAG may benefit from more frequent examinations and early preventive treatment.
Trial registration: clinicaltrials.gov Identifier: NCT00000125.
Figures







Comment in
-
Treatment of ocular hypertension: Hamlet's Lament revisited.Arch Ophthalmol. 2010 Mar;128(3):363-4. doi: 10.1001/archophthalmol.2010.13. Arch Ophthalmol. 2010. PMID: 20212209 No abstract available.
References
-
- Sommer A, Tielsch JM, Katz J, et al. Racial differences in the cause-specific prevalence of blindness in east Baltimore. N Engl J Med. 1991;325(20):1412–1417. - PubMed
-
- US Department of Health. Education, and Welfare. Statistics on blindness in the model reporting area 1969–1970. Washington, DC: US Government Printing Office; 1973.
-
- Quigley HA, Vitale S. Models of open-angle glaucoma prevalence and incidence in the United States. Invest Ophthalmol Vis Sci. 1997;38(1):83–91. - PubMed
-
- Hyman L, Wu SY, Connell AM, et al. Prevalence and causes of visual impairment in the Barbados Eye Study. Ophthalmology. 2001;108(10):1751–1756. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
