

Incidence of pediatric Horner syndrome and the risk of neuroblastoma: a population-based study
- PMID: 20212203
- PMCID: PMC3743544
- DOI: 10.1001/archophthalmol.2010.6
Incidence of pediatric Horner syndrome and the risk of neuroblastoma: a population-based study
Abstract
Objective: To describe the incidence of pediatric Horner syndrome and the risk of occult malignancy in a population-based cohort.
Methods: The medical records of all pediatric patients (aged <19 years) residing in Olmsted County, Minnesota, who received diagnoses of Horner syndrome from January 1, 1969, through December 31, 2008, were retrospectively reviewed.
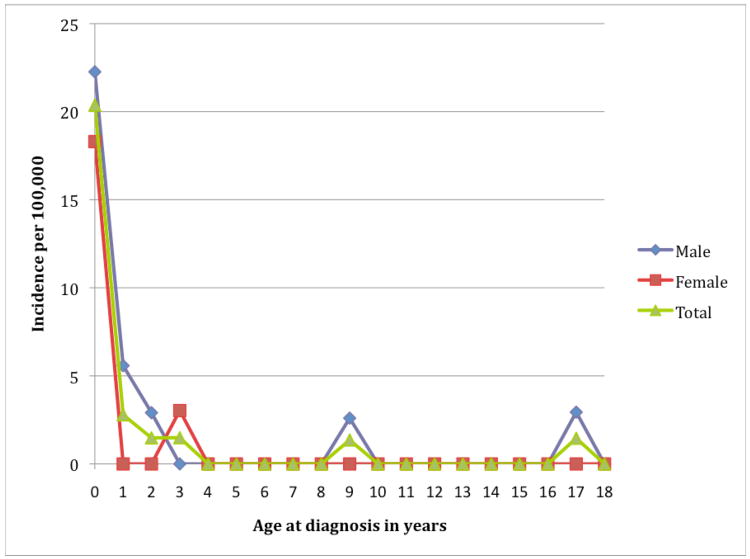
Results: Horner syndrome was diagnosed in 20 pediatric patients during the 40-year period, yielding an age- and sex-adjusted incidence of 1.42 per 100 000 patients younger than 19 years of age (95% confidence interval [CI], 0.80-2.04). Eleven of the 20 patients (55%) had a congenital onset, for a birth prevalence of 1 in 6250 (95% CI, 3333-10 000), while the remaining 9 (45%) had acquired syndromes. Seven of the 11 (63.6%) patients with congenital cases had a history of birth trauma, while the remaining 4 (36.4%) had no identifiable cause. Six of the 9 (66%) acquired cases occurred following surgery or trauma, while the remaining 3 (33%) had no known etiology. None of the 20 patients (95% CI, 0.0%-16.8%) were found to have a neuroblastoma or other malignancy during a mean follow-up of 56.5 months (range, 0-256.9 months).
Conclusions: The incidence of pediatric Horner syndrome in this population was 1.42 per 100 000 patients younger than 19 years, with a birth prevalence of 1 in 6250 for those with a congenital onset. Birth, surgical, or other trauma occurred in 13 (65%) of the patients, while none were found to have an underlying mass lesion, suggesting a need for reappraising current recommendations for extensive evaluations in these patients.
Figures
Comment in
-
Pediatric horner syndrome.Arch Ophthalmol. 2011 Aug;129(8):1108-9; author reply 1109. doi: 10.1001/archophthalmol.2011.201. Arch Ophthalmol. 2011. PMID: 21825206 No abstract available.
References
-
- Crippa SV, Borruat FX, Kawasaki A. Pupillary Dilation Lag is Intermittently Present in Patients With a Stable Oculosymathetic Defect (Horner Syndrome) Am J Ophthalmol. 2007;143:712–715. - PubMed
-
- Martin TJ. Horner's Syndrome, Pseudo-Horner's Syndrome, and Simple Anisocoria. Current Neurology and Neuroscience Reports. 2007;8:397–406. - PubMed
-
- Mahoney NR, Liu GT, Menacker SJ, et al. Pediatric Horner Syndrome: Etiologies and Roles of Imaging and Urine Studies to Detect Neuroblastoma and Other Responsible Mass Lesions. Am J Ophthalmol. 2006;142:651–659. - PubMed
-
- Jeffery AR, Ellis FJ, Repka MX, et al. Pediatric Horner Syndrome. J AAPOS. 1998;2:159–167. - PubMed
-
- Weinstein JM, Zweifel TJ, Thompson HS. Congenital Horner syndrome. Arch Ophthalmol. 1980;98:1074–1078. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
