

Relapse and late mortality in 5-year survivors of myeloablative allogeneic hematopoietic cell transplantation for chronic myeloid leukemia in first chronic phase
- PMID: 20212247
- PMCID: PMC2860369
- DOI: 10.1200/JCO.2009.26.7757
Relapse and late mortality in 5-year survivors of myeloablative allogeneic hematopoietic cell transplantation for chronic myeloid leukemia in first chronic phase
Abstract
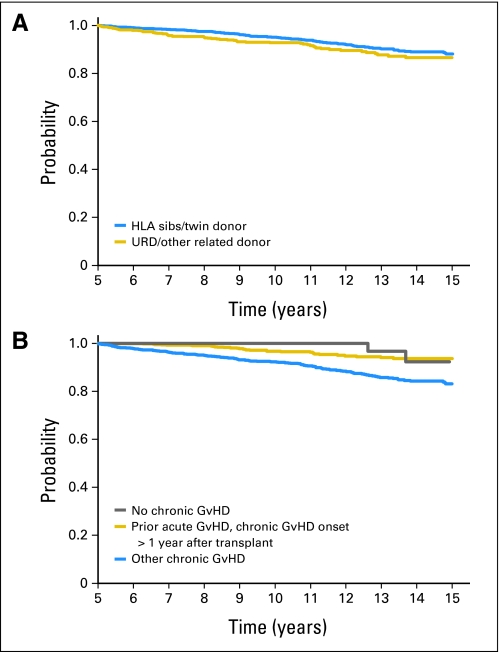
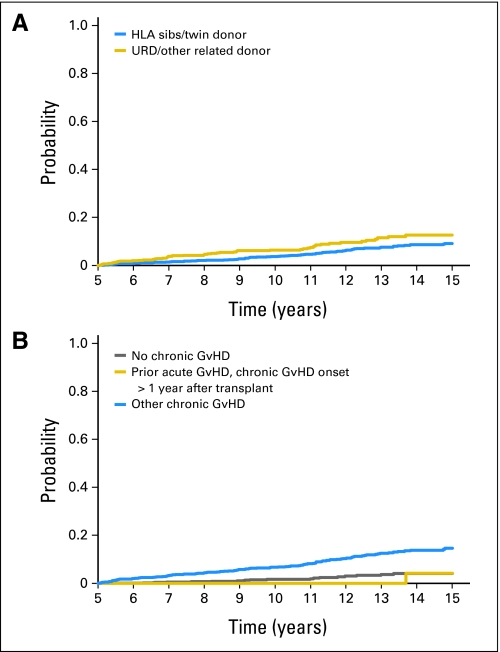
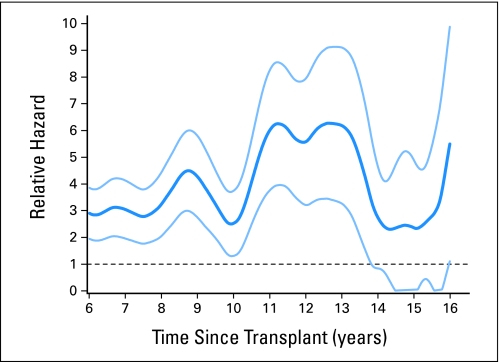
PURPOSE Allogeneic hematopoietic cell transplantation (HCT) is curative therapy for chronic myeloid leukemia (CML), but its long-term outcomes are not well described. We studied the long-term outcomes of CML patients in first chronic phase who receive an allogeneic HCT. PATIENTS AND METHODS Our study included 2,444 patients who received myeloablative HCT for CML in first chronic phase between 1978 and 1998 and survived in continuous complete remission for at least 5 years (median follow-up, 11 years; range, 5 to 25 years). Donor sources were human leukocyte antigen-matched siblings in 1,692 patients, unrelated donors in 639 patients, and other related donors in 113 patients. RESULTS Overall survival rates at 15 years were 88% (95% CI, 86% to 90%) for sibling HCT and 87% (95% CI, 83% to 90%) for unrelated donor HCT. Corresponding cumulative incidences of relapse were 8% (95% CI, 7% to 10%) and 2% (95% CI, 1% to 4%), respectively. The latest relapse was reported 18 years post-HCT. In multivariable analyses, history of chronic graft-versus-host disease increased risks of late overall mortality and nonrelapse mortality but reduced risks of relapse. In comparison with age-, race-, and sex-adjusted normal populations, the mortality of HCT recipients was significantly higher until 14 years post-HCT; thereafter, mortality rates were similar to those of the general population (relative mortality ratio at 15 years, 2.3; 95% CI, 0 to 4.9). CONCLUSION Recipients of allogeneic HCT for CML in first chronic phase who remain in remission for at least 5 years have favorable subsequent long-term survival, and their mortality rates eventually approach those of the general population.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Giralt SA, Arora M, Goldman JM, et al. Impact of imatinib therapy on the use of allogeneic haematopoietic progenitor cell transplantation for the treatment of chronic myeloid leukaemia. Br J Haematol. 2007;137:461–467. - PubMed
-
- Gale RP, Hehlmann R, Zhang MJ, et al. Survival with bone marrow transplantation versus hydroxyurea or interferon for chronic myelogenous leukemia. Blood. 1998;91:1810–1819. - PubMed
-
- Goldman JM. How I treat chronic myeloid leukemia in the imatinib era. Blood. 2007;110:2828–2837. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
