

Pharmacologically induced thoracic and abdominal aortic aneurysms in mice
- PMID: 20212272
- PMCID: PMC2859958
- DOI: 10.1161/HYPERTENSIONAHA.109.140558
Pharmacologically induced thoracic and abdominal aortic aneurysms in mice
Abstract
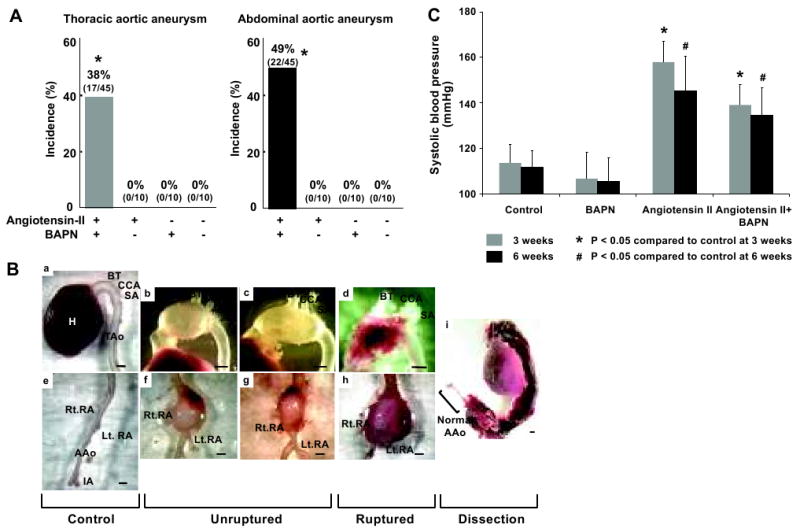
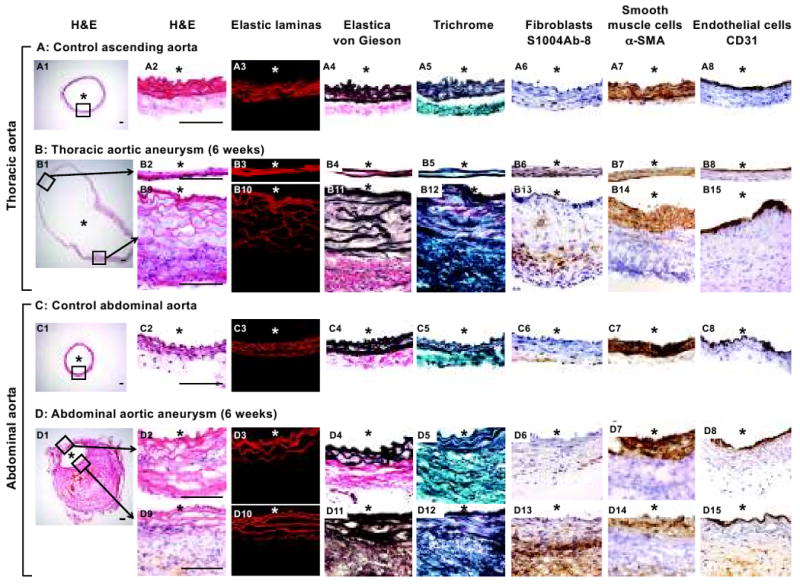
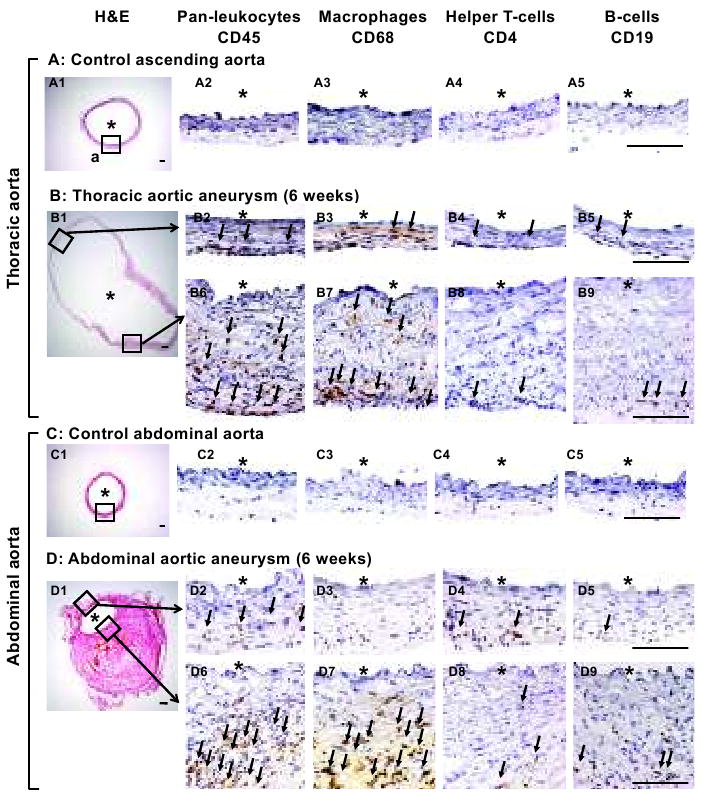
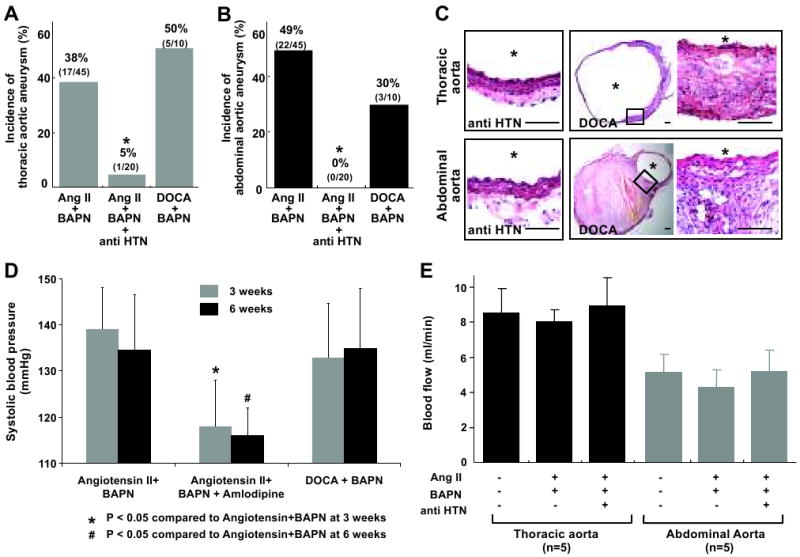
Aortic aneurysms are common among the elderly population. A large majority of aortic aneurysms are located at two distinct aneurysm-prone regions, the abdominal aorta and thoracic aorta involving the ascending aorta. In this study, we combined two factors that are associated with human aortic aneurysms, hypertension and degeneration of elastic lamina, to induce an aortic aneurysm in mice. Roles of hemodynamic conditions in the formation of aortic aneurysms were assessed using two different methods for inducing hypertension and antihypertensive agents. In 9-week-old C57BL/6J male mice, hypertension was induced by angiotensin II or deoxycorticosterone acetate-salt hypertension; degeneration of elastic lamina was induced by infusion of beta-aminopropionitrile, a lysyl oxidase inhibitor. Irrespective of the methods for inducing hypertension, mice developed thoracic and abdominal aortic aneurysms (38% to 50% and 30 to 49%, respectively). Aneurysms were found at the two aneurysm-prone regions with site-specific morphological and histological characteristics. Treatment with an antihypertensive agent, amlodipine, normalized blood pressure and dramatically reduced aneurysm formation in the mice that received angiotensin II and beta-aminopropionitrile. However, treatment with captopril, an angiotensin-converting enzyme inhibitor, did not affect blood pressure or the incidence of aortic aneurysms in the mice that received deoxycorticosterone acetate-salt and beta-aminopropionitrile. In summary, we have shown that a combination of hypertension and pharmacologically induced degeneration of elastic laminas can induce both thoracic and abdominal aortic aneurysms with site-specific characteristics. The aneurysm formation in this model depended on hypertension but not on direct effects of angiotensin II to the vascular wall.
Conflict of interest statement
Figures
References
-
- Axisa B, Loftus IM, Naylor AR, Goodall S, Jones L, Bell PR, Thompson MM. Prospective, randomized, double-blind trial investigating the effect of doxycycline on matrix metalloproteinase expression within atherosclerotic carotid plaques. Stroke. 2002;33:2858–2864. - PubMed
-
- Dapunt OE, Galla JD, Sadeghi AM, Lansman SL, Mezrow CK, de Asla RA, Quintana C, Wallenstein S, Ergin AM, Griepp RB. The natural history of thoracic aortic aneurysms. The Journal of thoracic and cardiovascular surgery. 1994;107:1323–1332. - PubMed
-
- Lederle FA, Johnson GR, Wilson SE, Chute EP, Littooy FN, Bandyk D, Krupski WC, Barone GW, Acher CW, Ballard DJ. Prevalence and associations of abdominal aortic aneurysm detected through screening. Aneurysm Detection and Management (ADAM) Veterans Affairs Cooperative Study Group. Ann Intern Med. 1997;126:441–449. - PubMed
-
- Tang PC, Coady MA, Lovoulos C, Dardik A, Aslan M, Elefteriades JA, Tellides G. Hyperplastic cellular remodeling of the media in ascending thoracic aortic aneurysms. Circulation. 2005;112:1098–1105. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
