

Effect of the AutoPulse automated band chest compression device on hemodynamics in out-of-hospital cardiac arrest resuscitation
- PMID: 20213073
- PMCID: PMC2929359
- DOI: 10.1007/s00134-010-1784-x
Effect of the AutoPulse automated band chest compression device on hemodynamics in out-of-hospital cardiac arrest resuscitation
Abstract
Purpose: Guidelines for advanced life support of cardiac arrest (CA) emphasize continuous and effective chest compressions as one of the main factors of cardiopulmonary resuscitation (CPR) success. The use of an automated load distributing chest compression device for CPR is promising but initial studies on survival show contradictory results. The aim of this study was to evaluate the effects of AutoPulse on blood pressure (BP) in out-of-hospital CA patients.
Methods: This prospective study included adult patients presenting with in refractory out-of-hospital CA. Invasive arterial BP produced by AutoPulse was compared to BP generated by manual CPR (Active Compression Decompression). Systolic, diastolic and mean BP and end-tidal carbon dioxide were recorded before and after initiating the automated band device for each patient. The comparison of diastolic BP produced by manual CPR versus automated chest compressions was the primary end point.
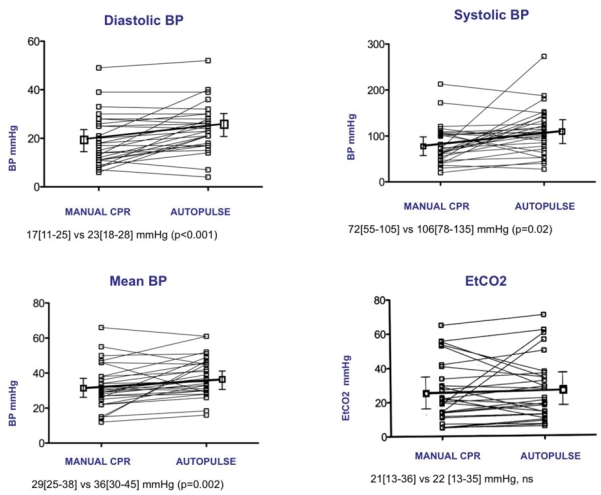
Results: Hemodynamics in 29 patients are reported and analyzed. Median diastolic BP increased after starting AutoPulse from 17[11-25] mmHg to 23[18-28] mmHg (P < 0.001). Median systolic BP increased from 72[55-105] mmHg to 106[78-135] mmHg (P = 0.02). Mean BP increased from 29[25-38] mmHg to 36[30-15] mmHg (P = 0.002). On the other hand, End-Tidal CO(2) did not increase significantly with AutoPulse (21[13-36] vs. 22[12-35] mmHg, P = 0.80).
Conclusions: In patients with out-of-hospital CA, the use of AutoPulse is associated with an increased diastolic BP compared to manual chest compressions. While its benefit to survival has yet to be demonstrated, the increase in diastolic and mean BP is a promising outcome for AutoPulse use.
Conflict of interest statement
No potential conflict of interest.
Figures
References
-
- Nolan JP, Deakin CD, Soar J, Böttiger BW, Smith G. European Resuscitation Council Guidelines for Resuscitation 2005, Section 4. Adult advanced life support. Resuscitation. 2005;67S1:S39–S86. - PubMed
-
- International Liaison Committee on Resuscitation. 2005 International Guidelines Conference on Cardiopulmonary Resuscitation and Emergency Care Science with Treatment Recommandations. Part 4: Advanced Life support. Resuscitation. 2005;67:213–247. - PubMed
-
- Delguercio LR, Feins NR, Cohn JD, Coomaraswamy RP, Wollman SB, State D. Comparison of blood flow during external and internal cardiac massage in man. Circulation. 1965;31:171–180. - PubMed
-
- Wik L, Kramer-Johansen J, Myklebust H, et al. Quality of cardiopulmonary resuscitation during out-of-hospital cardiac arrest. JAMA. 2005;293:299–304. - PubMed
