

Is sequential cranial ultrasound reliable for detection of white matter injury in very preterm infants?
- PMID: 20213135
- PMCID: PMC2852528
- DOI: 10.1007/s00234-010-0668-7
Is sequential cranial ultrasound reliable for detection of white matter injury in very preterm infants?
Abstract
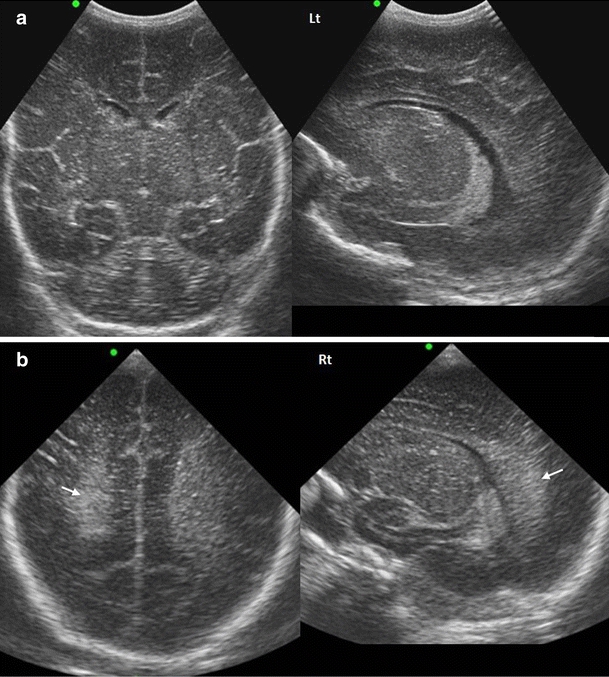
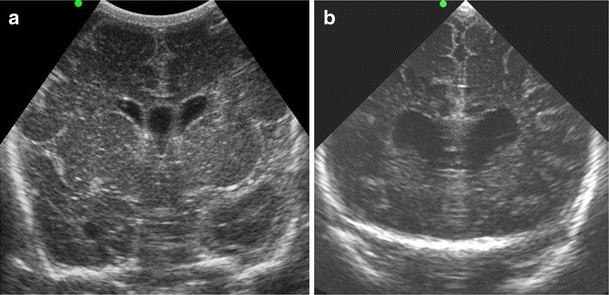
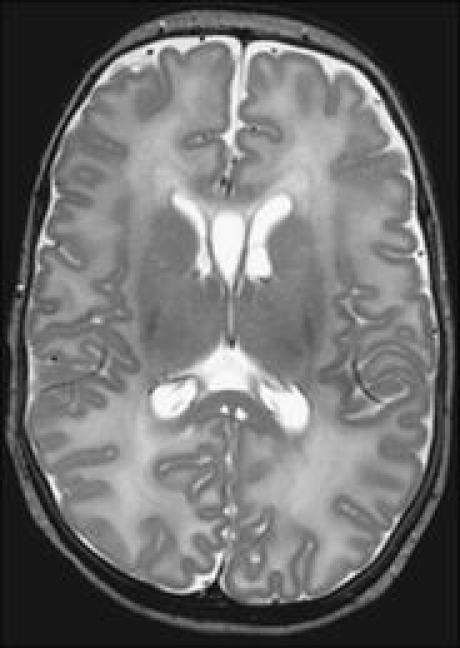
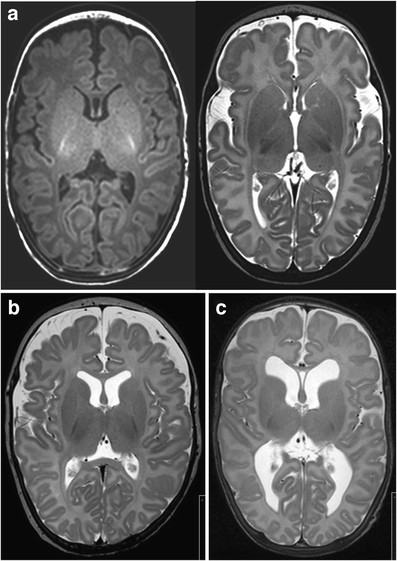
Introduction: Cranial ultrasound (cUS) may not be reliable for detection of diffuse white matter (WM) injury. Our aim was to assess in very preterm infants the reliability of a classification system for WM injury on sequential cUS throughout the neonatal period, using magnetic resonance imaging (MRI) as reference standard.
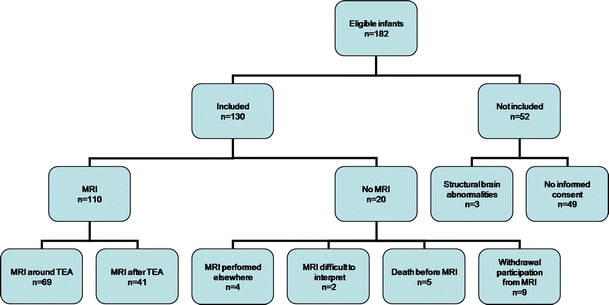
Methods: In 110 very preterm infants (gestational age <32 weeks), serial cUS during admission (median 8, range 4-22) and again around term equivalent age (TEA) and a single MRI around TEA were performed. cUS during admission were assessed for presence of WM changes, and contemporaneous cUS and MRI around TEA additionally for abnormality of lateral ventricles. Sequential cUS (from birth up to TEA) and MRI were classified as normal/mildly abnormal, moderately abnormal, or severely abnormal, based on a combination of findings of the WM and lateral ventricles. Predictive values of the cUS classification were calculated.
Results: Sequential cUS were classified as normal/mildly abnormal, moderately abnormal, and severely abnormal in, respectively, 22%, 65%, and 13% of infants and MRI in, respectively, 30%, 52%, and 18%. The positive predictive value of the cUS classification for the MRI classification was high for severely abnormal WM (0.79) but lower for normal/mildly abnormal (0.67) and moderately abnormal (0.64) WM.
Conclusion: Sequential cUS during the neonatal period detects severely abnormal WM in very preterm infants but is less reliable for mildly and moderately abnormal WM. MRI around TEA seems needed to reliably detect WM injury in very preterm infants.
Figures


Similar articles
-
Comparison of cranial ultrasound and MRI for detecting BRAIN injury in extremely preterm infants and correlation with neurological outcomes at 1 and 3 years.Eur J Pediatr. 2019 Jul;178(7):1053-1061. doi: 10.1007/s00431-019-03388-7. Epub 2019 May 7. Eur J Pediatr. 2019. PMID: 31065842
-
Comparing brain white matter on sequential cranial ultrasound and MRI in very preterm infants.Neuroradiology. 2008 Sep;50(9):799-811. doi: 10.1007/s00234-008-0408-4. Epub 2008 Jun 11. Neuroradiology. 2008. PMID: 18545992
-
Cranial ultrasound and MRI at term age in extremely preterm infants.Arch Dis Child Fetal Neonatal Ed. 2010 Sep;95(5):F310-4. doi: 10.1136/adc.2009.161547. Epub 2009 Oct 19. Arch Dis Child Fetal Neonatal Ed. 2010. PMID: 19843500
-
Preterm white matter injury: ultrasound diagnosis and classification.Pediatr Res. 2020 Mar;87(Suppl 1):37-49. doi: 10.1038/s41390-020-0781-1. Pediatr Res. 2020. PMID: 32218534 Free PMC article. Review.
-
Neuroimaging of white matter injury, intraventricular and cerebellar hemorrhage.Clin Perinatol. 2014 Mar;41(1):69-82. doi: 10.1016/j.clp.2013.09.005. Epub 2013 Dec 17. Clin Perinatol. 2014. PMID: 24524447 Review.
Cited by
-
Rate of head ultrasound abnormalities at one month in very premature and extremely premature infants with normal initial screening ultrasound.Pediatr Radiol. 2022 May;52(6):1150-1157. doi: 10.1007/s00247-022-05285-y. Epub 2022 Jan 31. Pediatr Radiol. 2022. PMID: 35102433 Free PMC article.
-
Comparing 3T T1-weighted sequences in identifying hyperintense punctate lesions in preterm neonates.AJNR Am J Neuroradiol. 2015 Mar;36(3):581-6. doi: 10.3174/ajnr.A4144. Epub 2014 Nov 6. AJNR Am J Neuroradiol. 2015. PMID: 25376807 Free PMC article.
-
Neurocritical care for neonates.Curr Treat Options Neurol. 2011 Dec;13(6):574-89. doi: 10.1007/s11940-011-0144-7. Curr Treat Options Neurol. 2011. PMID: 21874296
-
Comparison of cranial ultrasound and MRI for detecting BRAIN injury in extremely preterm infants and correlation with neurological outcomes at 1 and 3 years.Eur J Pediatr. 2019 Jul;178(7):1053-1061. doi: 10.1007/s00431-019-03388-7. Epub 2019 May 7. Eur J Pediatr. 2019. PMID: 31065842
-
Quantitative ultrasonographic examination of cerebral white matter by pixel brightness intensity as marker of middle-term neurodevelopment: a prospective observational study.Sci Rep. 2023 Oct 5;13(1):16816. doi: 10.1038/s41598-023-44083-w. Sci Rep. 2023. PMID: 37798394 Free PMC article.
References
-
- Paneth N, Rudelli R, Monte W, Rodriguez E, Pinto J, Kairam R, Kazam E. White matter necrosis in very low birth weight infants: neuropathologic and ultrasonographic findings in infants surviving six days or longer. J Pediatr. 1990;16:975–984. - PubMed
-
- Cornette LG, Tanner SF, Ramenghi LA, Miall LS, Childs AM, Arthur RJ, Martinez D, Levene MI. Magnetic resonance imaging of the infant brain: anatomical characteristics and clinical significance of punctate lesions. Arch Dis Child Fetal Neonatal Ed. 2002;86:F171–F177. doi: 10.1136/fn.86.3.F171. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
