

Intralesional hemorrhage and thrombosis without rupture in a pure spinal epidural cavernous angioma: a rare cause of acute lumbal radiculopathy
- PMID: 20213297
- PMCID: PMC2899646
- DOI: 10.1007/s00586-010-1345-6
Intralesional hemorrhage and thrombosis without rupture in a pure spinal epidural cavernous angioma: a rare cause of acute lumbal radiculopathy
Abstract
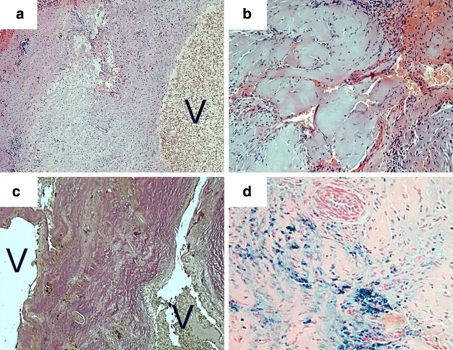
Pure spinal epidural cavernous angiomas are extremely rare lesions, and their normal shape is that of a fusiform mass in the dorsal aspects of the spinal canal. We report a case of a lumbo-sacral epidural cavernous vascular malformation presenting with acute onset of right-sided S1 radiculopathy. Clinical aspects, imaging, intraoperative findings, and histology are demonstrated. The patient, a 27-year-old man presented with acute onset of pain, paraesthesia, and numbness within the right leg corresponding to the S1 segment. An acute lumbosacral disc herniation was suspected, but MRI revealed a cystic lesion with the shape of a balloon, a fluid level and a thickened contrast-enhancing wall. Intraoperatively, a purple-blue tumor with fibrous adhesions was located between the right S1 and S2 nerve roots. Macroscopically, no signs of epidural bleedings could be denoted. After coagulation of a reticular venous feeder network and dissection of the adhesions the rubber ball-like lesion was resected in total. Histology revealed a prominent venous vessel with a pathologically thickened, amuscular wall surrounded by smaller, hyalinized, venous vessels arranged in a back-to-back position typical for the diagnosis of a cavernous angioma. Lumina were partially occluded by thrombi. The surrounding fibrotic tissue showed signs of recurrent bleedings. There was no obvious mass hemorrhage into the surrounding tissue. In this unique case, the pathologic mechanism was not the usual rupture of the cavernous angioma with subsequent intraspinal hemorrhage, but acute mass effect by intralesional bleedings and thrombosis with subsequent increase of volume leading to nerve root compression. Thus, even without a sudden intraspinal hemorrhage a spinal cavernous malformation can cause acute symptoms identical to the clinical features of a soft disc herniation.
Figures

Similar articles
-
Solitary spinal epidural cavernous angiomas in children presenting with acute neurological symptoms caused by hemorrhage.J Neurosurg Pediatr. 2010 Jan;5(1):89-93. doi: 10.3171/2009.7.PEDS09203. J Neurosurg Pediatr. 2010. PMID: 20043742
-
Pure epidural cavernous hemangioma of the cervical spine that presented with an acute sensory deficit caused by hemorrhage.Yonsei Med J. 2006 Dec 31;47(6):877-80. doi: 10.3349/ymj.2006.47.6.877. Yonsei Med J. 2006. PMID: 17191320 Free PMC article.
-
Spontaneous hemorrhage into a lumbar synovial cyst.Eur Spine J. 2010 Jul;19 Suppl 2(Suppl 2):S190-2. doi: 10.1007/s00586-010-1332-y. Epub 2010 Feb 21. Eur Spine J. 2010. PMID: 20174835 Free PMC article.
-
Extreme lateral lumbar disc herniation in a 12-year child: case report and review of the literature.Eur Spine J. 2010 Jul;19 Suppl 2(Suppl 2):S197-9. doi: 10.1007/s00586-010-1354-5. Epub 2010 Mar 10. Eur Spine J. 2010. PMID: 20221778 Free PMC article. Review.
-
[Epidural varicosis as a rare cause of acute radiculopathy with complete foot paresis--case report and literature review].Z Orthop Ihre Grenzgeb. 2007 Jan-Feb;145(1):55-60. doi: 10.1055/s-2007-960503. Z Orthop Ihre Grenzgeb. 2007. PMID: 17345544 Review. German.
Cited by
-
Lumbar Epidural Cavernous Hemangioma: A Case Report and Review of the Literature.Cureus. 2023 Jan 12;15(1):e33677. doi: 10.7759/cureus.33677. eCollection 2023 Jan. Cureus. 2023. PMID: 36788892 Free PMC article.
-
Thoracic extraosseous, epidural, cavernous hemangioma: Case report and review of literature.J Neurosci Rural Pract. 2013 Jul;4(3):309-12. doi: 10.4103/0976-3147.118772. J Neurosci Rural Pract. 2013. PMID: 24250167 Free PMC article.
-
Pure extraosseous spinal epidural cavernous hemangioma presenting with acute paraplegia: a case report.Spinal Cord Ser Cases. 2022 Jun 30;8(1):63. doi: 10.1038/s41394-022-00531-9. Spinal Cord Ser Cases. 2022. PMID: 35773281 Free PMC article.
-
A rare case of thoracic extradural thrombosed primary cavernous haemangioma in a relatively asymptomatic patient.Surg Neurol Int. 2014 Dec 15;5:180. doi: 10.4103/2152-7806.146962. eCollection 2014. Surg Neurol Int. 2014. PMID: 25593764 Free PMC article. No abstract available.
-
Clinical and radiological presentation of spinal epidural haemangiomas: clinical series in a tertiary care centre during a 10-year period.Eur Spine J. 2014 Feb;23(2):404-10. doi: 10.1007/s00586-013-3045-5. Epub 2013 Oct 6. Eur Spine J. 2014. PMID: 24097259 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
