

Chapter 7. Critical care triage. Recommendations and standard operating procedures for intensive care unit and hospital preparations for an influenza epidemic or mass disaster
- PMID: 20213422
- PMCID: PMC4849534
- DOI: 10.1007/s00134-010-1765-0
Chapter 7. Critical care triage. Recommendations and standard operating procedures for intensive care unit and hospital preparations for an influenza epidemic or mass disaster
Abstract
Purpose: To provide recommendations and standard operating procedures for intensive care unit (ICU) and hospital preparations for an influenza pandemic or mass disaster with a specific focus on critical care triage.
Methods: Based on a literature review and expert opinion, a Delphi process was used to define the essential topics including critical care triage.
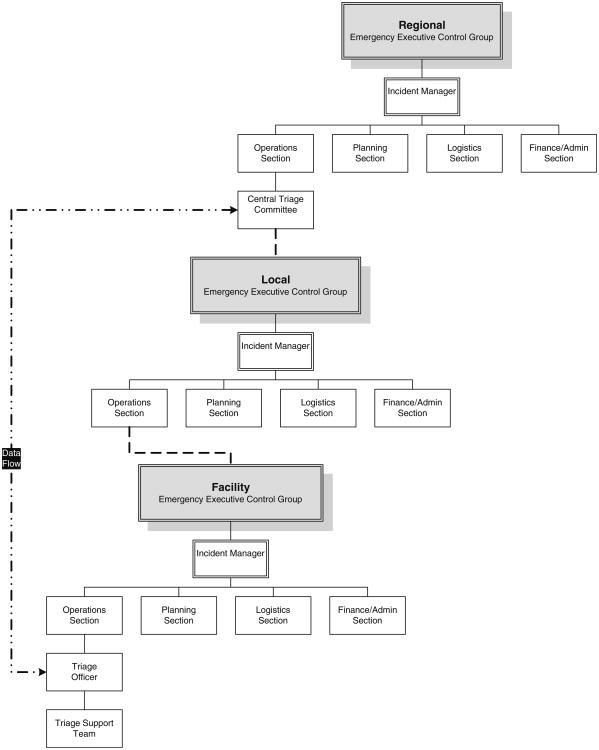
Results: Key recommendations include: (1) establish an Incident Management System with Emergency Executive Control Groups at facility, local, regional/state or national levels to exercise authority and direction over resources; (2) developing fair and equitable policies may require restricting ICU services to patients most likely to benefit; (3) usual treatments and standards of practice may be impossible to deliver; (4) ICU care and treatments may have to be withheld from patients likely to die even with ICU care and withdrawn after a trial in patients who do not improve or deteriorate; (5) triage criteria should be objective, ethical, transparent, applied equitably and be publically disclosed; (6) trigger triage protocols for pandemic influenza only when critical care resources across a broad geographic area are or will be overwhelmed despite all reasonable efforts to extend resources or obtain additional resources; (7) triage of patients for ICU should be based on those who are likely to benefit most or a 'first come, first served' basis; (8) a triage officer should apply inclusion and exclusion criteria to determine patient qualification for ICU admission.
Conclusions: Judicious planning and adoption of protocols for critical care triage are necessary to optimize outcomes during a pandemic.
Conflict of interest statement
The views expressed in the paper are those of the authors and do not reflect policies of the US Department of Health and Human Services or the National Institutes of Health or the Department of National Defence/Canadian Forces.
Figures
Similar articles
-
Chapter 3. Coordination and collaboration with interface units. Recommendations and standard operating procedures for intensive care unit and hospital preparations for an influenza epidemic or mass disaster.Intensive Care Med. 2010 Apr;36 Suppl 1(Suppl 1):S21-31. doi: 10.1007/s00134-010-1762-3. Intensive Care Med. 2010. PMID: 20213418 Free PMC article.
-
Recommendations for intensive care unit and hospital preparations for an influenza epidemic or mass disaster: summary report of the European Society of Intensive Care Medicine's Task Force for intensive care unit triage during an influenza epidemic or mass disaster.Intensive Care Med. 2010 Mar;36(3):428-43. doi: 10.1007/s00134-010-1759-y. Epub 2010 Feb 5. Intensive Care Med. 2010. PMID: 20135090 Free PMC article. Review.
-
Chapter 2. Surge capacity and infrastructure considerations for mass critical care. Recommendations and standard operating procedures for intensive care unit and hospital preparations for an influenza epidemic or mass disaster.Intensive Care Med. 2010 Apr;36 Suppl 1:S11-20. doi: 10.1007/s00134-010-1761-4. Intensive Care Med. 2010. PMID: 20213417
-
Chapter 9. Educational process. Recommendations and standard operating procedures for intensive care unit and hospital preparations for an influenza epidemic or mass disaster.Intensive Care Med. 2010 Apr;36 Suppl 1(Suppl 1):S70-9. doi: 10.1007/s00134-010-1768-x. Intensive Care Med. 2010. PMID: 20213424 Free PMC article.
-
Clinical review: mass casualty triage--pandemic influenza and critical care.Crit Care. 2007;11(2):212. doi: 10.1186/cc5732. Crit Care. 2007. PMID: 17490495 Free PMC article. Review.
Cited by
-
The Critical Care Society of Southern Africa Consensus Statement on ICU Triage and Rationing (ConICTri).South Afr J Crit Care. 2019 Aug 15;35(1b):10.7196/SAJCC.2019.v35.i1b.383. doi: 10.7196/SAJCC.2019.v35.i1b.383. eCollection 2019. South Afr J Crit Care. 2019. PMID: 37719327 Free PMC article.
-
Triage.Crit Care Clin. 2019 Oct;35(4):575-589. doi: 10.1016/j.ccc.2019.06.009. Epub 2019 Jul 27. Crit Care Clin. 2019. PMID: 31445606 Free PMC article. Review.
-
Triage protocol for allocation of critical health resources during Covid-19 pandemic and public health emergencies. A narrative review.Acta Biomed. 2020 Nov 10;91(4):e2020162. doi: 10.23750/abm.v91i4.10393. Acta Biomed. 2020. PMID: 33525236 Free PMC article. Review.
-
Critical care and pandemic preparedness and response.Br J Anaesth. 2023 Nov;131(5):847-860. doi: 10.1016/j.bja.2023.07.026. Epub 2023 Sep 14. Br J Anaesth. 2023. PMID: 37689541 Free PMC article. Review.
-
The Simple Triage Scoring System (STSS) successfully predicts mortality and critical care resource utilization in H1N1 pandemic flu: a retrospective analysis.Crit Care. 2011;15(1):R39. doi: 10.1186/cc10001. Epub 2011 Jan 26. Crit Care. 2011. PMID: 21269458 Free PMC article.
References
-
- Vollmar LC. Military medicine in war: the Geneva Conventions today. In: Beam TE, Sparacino LR, editors. Military medical ethics. Office of The Surgeon General Department of the Army, USA; 2003.
-
- Benson M, Koenig KL, Schultz CH. Disaster triage: START, then SAVE–a new method of dynamic triage for victims of a catastrophic earthquake. Prehosp Disaster Med. 1996;11:117–124. - PubMed
-
- Garner A, Lee A, Harrison K, Schultz CH. Comparative analysis of multiple-casualty incident triage algorithms. Ann Emerg Med. 2001;38:541–548. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
