

Acute gonadotroph and somatotroph hormonal suppression after traumatic brain injury
- PMID: 20214417
- PMCID: PMC2943504
- DOI: 10.1089/neu.2009.1092
Acute gonadotroph and somatotroph hormonal suppression after traumatic brain injury
Abstract
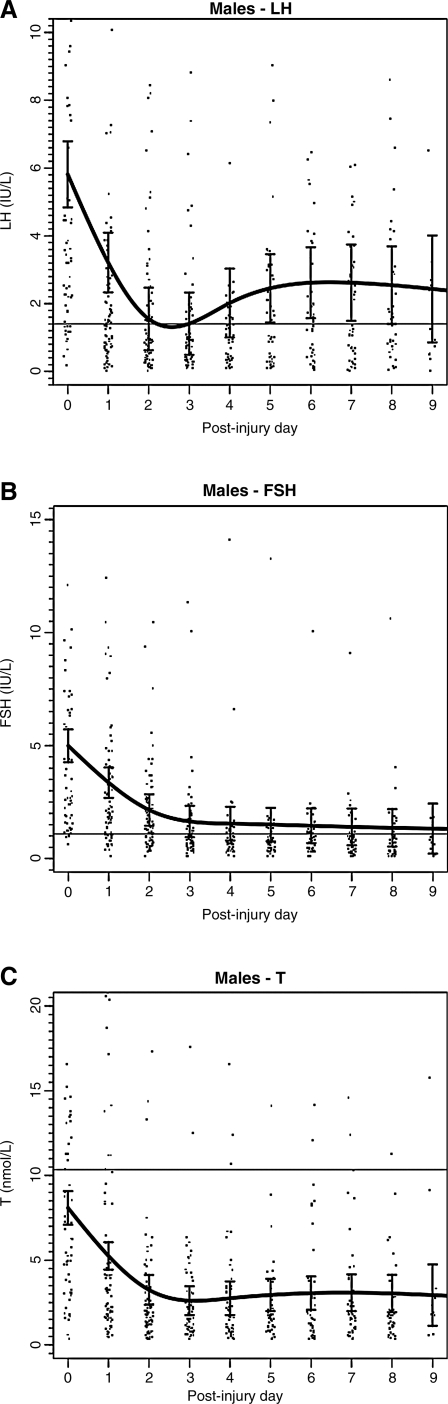
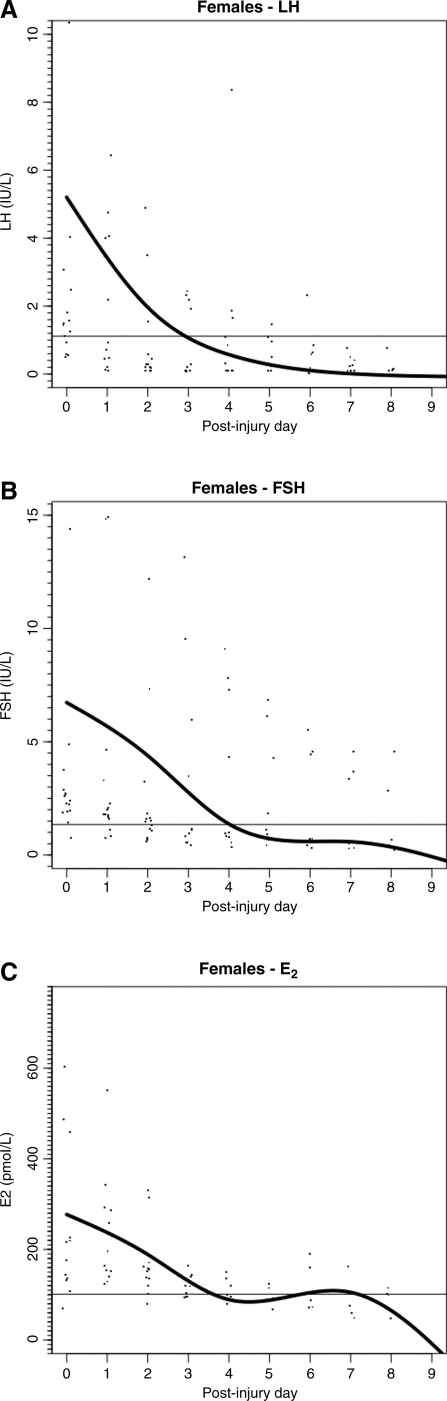
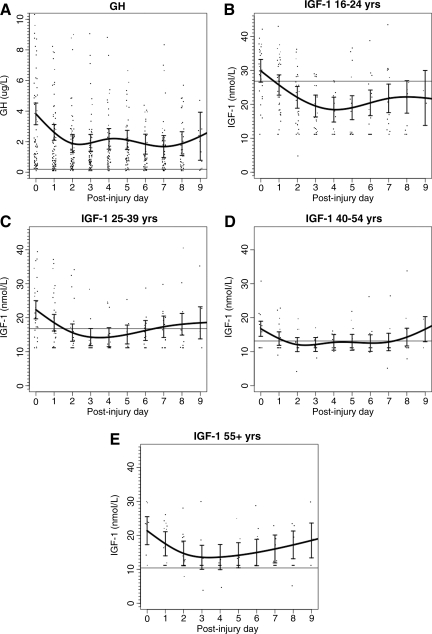
Hormonal dysfunction is a known consequence of moderate and severe traumatic brain injury (TBI). In this study we determined the incidence, time course, and clinical correlates of acute post-TBI gonadotroph and somatotroph dysfunction. Patients had daily measurement of serum luteinizing hormone (LH), follicle-stimulating hormone (FSH), testosterone, estradiol, growth hormone, and insulin-like growth factor-1 (IGF-1) for up to 10 days post-injury. Values below the fifth percentile of a healthy cohort were considered abnormal, as were non-measurable growth hormone (GH) values. Outcome measures were frequency and time course of hormonal suppression, injury characteristics, and Glasgow Outcome Scale (GOS) score. The cohort consisted of 101 patients (82% males; mean age 35 years; Glasgow Coma Scale [GCS] score <or=8 in 87%). In men, 100% had at least one low testosterone value, and 93% of all values were low; in premenopausal women, 43% had at least one low estradiol value, and 39% of all values were low. Non-measurable GH levels occurred in 38% of patients, while low IGF-1 levels were observed in 77% of patients, but tended to normalize within 10 days. Multivariate analysis revealed associations of younger age with low FSH and low IGF-1, acute anemia with low IGF-1, and older age and higher body mass index (BMI) with low GH. Hormonal suppression was not predictive of GOS score. These results indicate that within 10 days of complicated mild, moderate, and severe TBI, testosterone suppression occurs in all men and estrogen suppression occurs in over 40% of women. Transient somatotroph suppression occurs in over 75% of patients. Although this acute neuroendocrine dysfunction may not be TBI-specific, low gonadal steroids, IGF-1, and GH may be important given their putative neuroprotective functions.
Figures
Similar articles
-
Role of hormonal levels on hospital mortality for male patients with severe traumatic brain injury.Brain Inj. 2014;28(10):1262-9. doi: 10.3109/02699052.2014.915986. Epub 2014 May 19. Brain Inj. 2014. PMID: 24841415
-
Prevalence of anterior pituitary insufficiency 3 and 12 months after traumatic brain injury.Eur J Endocrinol. 2006 Feb;154(2):259-65. doi: 10.1530/eje.1.02071. Eur J Endocrinol. 2006. PMID: 16452539
-
Predictors of anterior pituitary insufficiency after traumatic brain injury.Clin Endocrinol (Oxf). 2008 Feb;68(2):206-12. doi: 10.1111/j.1365-2265.2007.03020.x. Epub 2007 Sep 4. Clin Endocrinol (Oxf). 2008. PMID: 17803694
-
Alterations of the GH/IGF-I Axis and Gut Microbiome after Traumatic Brain Injury: A New Clinical Syndrome?J Clin Endocrinol Metab. 2020 Sep 1;105(9):dgaa398. doi: 10.1210/clinem/dgaa398. J Clin Endocrinol Metab. 2020. PMID: 32585029 Review.
-
Neurotrophic and Neuroregenerative Effects of GH/IGF1.Int J Mol Sci. 2017 Nov 17;18(11):2441. doi: 10.3390/ijms18112441. Int J Mol Sci. 2017. PMID: 29149058 Free PMC article. Review.
Cited by
-
Systematic Review of Sex and Gender Effects in Traumatic Brain Injury: Equity in Clinical and Functional Outcomes.Front Neurol. 2021 Sep 10;12:678971. doi: 10.3389/fneur.2021.678971. eCollection 2021. Front Neurol. 2021. PMID: 34566834 Free PMC article.
-
Critical illness and sex hormones: response and impact of the hypothalamic-pituitary-gonadal axis.Ther Adv Endocrinol Metab. 2025 Apr 2;16:20420188251328192. doi: 10.1177/20420188251328192. eCollection 2025. Ther Adv Endocrinol Metab. 2025. PMID: 40183031 Free PMC article. Review.
-
Protective role of testosterone in ischemia-reperfusion-induced acute kidney injury.Am J Physiol Regul Integr Comp Physiol. 2013 Jun 1;304(11):R951-8. doi: 10.1152/ajpregu.00360.2012. Epub 2013 Apr 3. Am J Physiol Regul Integr Comp Physiol. 2013. PMID: 23552495 Free PMC article.
-
Sex Differences in Sex Hormone Profiles and Prediction of Consciousness Recovery After Severe Traumatic Brain Injury.Front Endocrinol (Lausanne). 2019 Apr 26;10:261. doi: 10.3389/fendo.2019.00261. eCollection 2019. Front Endocrinol (Lausanne). 2019. PMID: 31080439 Free PMC article.
-
Pathophysiology of Pediatric Traumatic Brain Injury.Front Neurol. 2021 Jul 15;12:696510. doi: 10.3389/fneur.2021.696510. eCollection 2021. Front Neurol. 2021. PMID: 34335452 Free PMC article. Review.
References
-
- Consensus conference. Rehabilitation of persons with traumatic brain injury. NIH Consensus Development Panel on Rehabilitation of Persons With Traumatic Brain Injury. JAMA. 1999;282:974–983. - PubMed
-
- Adekoya N. Thurman D.J. White D.D. Webb K.W. Surveillance for traumatic brain injury deaths—United States, 1989–1998. MMWR Surveill. Summ. 2002;51:1–14. - PubMed
-
- Agha A. Rogers B. Mylotte D. Taleb F. Tormey W. Phillips J. Thompson C.J. Neuroendocrine dysfunction in the acute phase of traumatic brain injury. Clin. Endocrinol. (Oxf.) 2004;60:584–591. - PubMed
-
- Albanese J. Martin C. Lacarelle B. Saux P. Durand A. Gouin F. Pharmacokinetics of long-term propofol infusion used for sedation in ICU patients. Anesthesiology. 1990;73:214–217. - PubMed
-
- Allen N.E. Appleby P.N. Davey G.K. Key T.J. Lifestyle and nutritional determinants of bioavailable androgens and related hormones in British men. Cancer Causes Control. 2002;13:353–363. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
