

Long-term impact of respiratory viral infection after pediatric lung transplantation
- PMID: 20214745
- PMCID: PMC2893330
- DOI: 10.1111/j.1399-3046.2010.01296.x
Long-term impact of respiratory viral infection after pediatric lung transplantation
Abstract
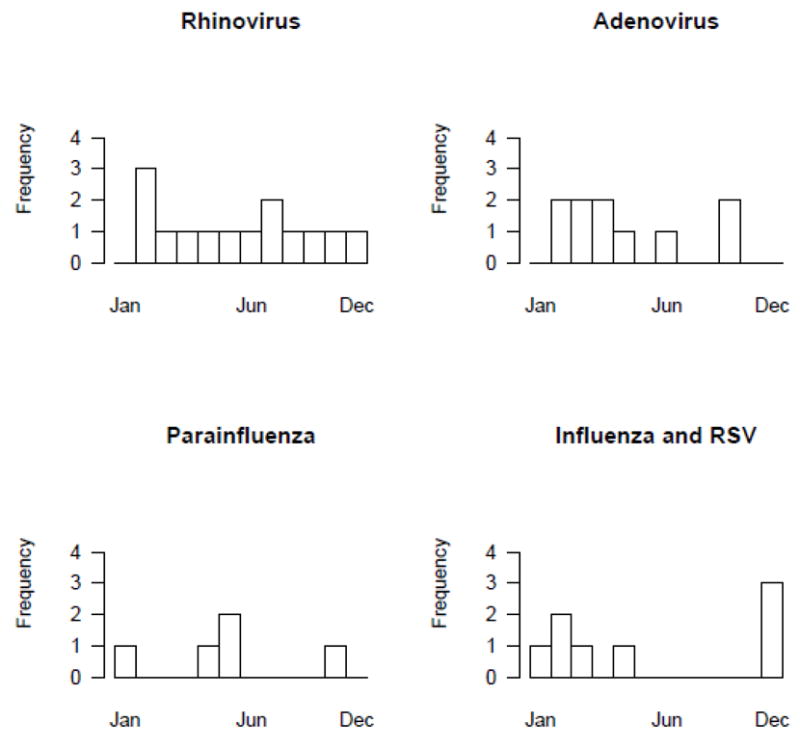
To evaluate the epidemiology and to investigate the impact of RVI on chronic allograft rejection after pediatric lung transplantation, a retrospective study of pediatric lung transplant recipients from 2002 to 2007 was conducted. Association between RVI and continuous and categorical risk factors was assessed using Wilcoxon rank-sum tests and Fisher's exact tests, respectively. Association between risk factors and outcomes were assessed using Cox proportional hazards models. Fifty-five subjects were followed for a mean of 674 days (range 14-1790). Twenty-eight (51%) developed 51 RVI at a median of 144 days post-transplant (mean 246; range 1-1276); 41% of infections were diagnosed within 90 days. Twenty-five subjects developed 39 LRI, and eight subjects had 11 URI. Organisms recovered included rhinovirus (n = 14), adenovirus (n = 10), parainfluenza (n = 10), influenza (n = 5), and RSV (n = 4). Three subjects expired secondary to their RVI (two adenovirus, one RSV). Younger age and prior CMV infection were risks for RVI (HR 2.4 95% CI 1.1-5.3 and 17.0; 3.0-96.2, respectively). RVI was not associated with the development of chronic allograft rejection (p = 0.25) or death during the study period. RVI occurs in the majority of pediatric lung transplant recipients, but was not associated with mortality or chronic allograft rejection.
Figures
Similar articles
-
A Multicenter Consortium to Define the Epidemiology and Outcomes of Pediatric Solid Organ Transplant Recipients With Inpatient Respiratory Virus Infection.J Pediatric Infect Dis Soc. 2019 Jul 1;8(3):197-204. doi: 10.1093/jpids/piy024. J Pediatric Infect Dis Soc. 2019. PMID: 29538674 Free PMC article.
-
Respiratory viral infections within one year after pediatric lung transplant.Transpl Infect Dis. 2009 Aug;11(4):304-12. doi: 10.1111/j.1399-3062.2009.00397.x. Epub 2009 May 3. Transpl Infect Dis. 2009. PMID: 19422670 Free PMC article.
-
Symptomatic Respiratory Virus Infection and Chronic Lung Allograft Dysfunction.Clin Infect Dis. 2016 Feb 1;62(3):313-319. doi: 10.1093/cid/civ871. Epub 2015 Nov 12. Clin Infect Dis. 2016. PMID: 26565010 Free PMC article.
-
[Infection in lung transplantation].Enferm Infecc Microbiol Clin. 2007 Dec;25(10):639-49; quiz 650. doi: 10.1157/13112940. Enferm Infecc Microbiol Clin. 2007. PMID: 18053475 Free PMC article. Review. Spanish.
-
Respiratory viral infections in transplant recipients.Antivir Ther. 2007;12(4 Pt B):627-38. Antivir Ther. 2007. PMID: 17944270 Review.
Cited by
-
Adenovirus infections in immunocompetent and immunocompromised patients.Clin Microbiol Rev. 2014 Jul;27(3):441-62. doi: 10.1128/CMR.00116-13. Clin Microbiol Rev. 2014. PMID: 24982316 Free PMC article. Review.
-
Rhinovirus induces an anabolic reprogramming in host cell metabolism essential for viral replication.Proc Natl Acad Sci U S A. 2018 Jul 24;115(30):E7158-E7165. doi: 10.1073/pnas.1800525115. Epub 2018 Jul 9. Proc Natl Acad Sci U S A. 2018. PMID: 29987044 Free PMC article.
-
Adenovirus: current epidemiology and emerging approaches to prevention and treatment.Curr Infect Dis Rep. 2014 Aug;16(8):416. doi: 10.1007/s11908-014-0416-y. Curr Infect Dis Rep. 2014. PMID: 24908344
-
A Multicenter Consortium to Define the Epidemiology and Outcomes of Pediatric Solid Organ Transplant Recipients With Inpatient Respiratory Virus Infection.J Pediatric Infect Dis Soc. 2019 Jul 1;8(3):197-204. doi: 10.1093/jpids/piy024. J Pediatric Infect Dis Soc. 2019. PMID: 29538674 Free PMC article.
-
Epidemiology and persistence of rhinovirus in pediatric lung transplantation.Transpl Infect Dis. 2020 Dec;22(6):e13422. doi: 10.1111/tid.13422. Epub 2020 Aug 2. Transpl Infect Dis. 2020. PMID: 32686323 Free PMC article.
References
-
- Waltz DA, Boucek MM, Edwards LB, Keck BM, Trulock EP, Taylor DO, et al. Registry of the International Society for Heart and Lung Transplantation: ninth official pediatric lung and heart-lung transplantation report--2006. J Heart Lung Transplant. 2006;25(8):904–911. - PubMed
-
- Kanj SS, Tapson V, Davis DR, Madden J, Browning I. Infections in Patients with Cystic Fibrosis following Lung Transplantation. Chest. 1997;112(4):924–930. - PubMed
-
- Kramer MR, Marshall SE, Starnes VA, Gamberg P, Amitai Z, Theodore J. Infectious complications in heart-lung transplant. Archives of Internal Medicine. 1993;153:2010–2016. - PubMed
-
- Maurer JR, Tullis DE, Grossman RF, Vellend H, Winton Tl, Patterson GA. Infectious complications following isolated lung transplant. Chest. 1992;101:1056–1059. - PubMed
-
- Milstone AP, Brumble LM, Barnes J, Estes W, Loyd JE, Pierson RN, 3rd, et al. A single-season prospective study of respiratory viral infections in lung transplant recipients. Eur Respir J. 2006;28(1):131–137. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
