

Substrate and Trigger Ablation for Reduction of Atrial Fibrillation (STAR AF): a randomized, multicentre, international trial
- PMID: 20215126
- PMCID: PMC2878965
- DOI: 10.1093/eurheartj/ehq041
Substrate and Trigger Ablation for Reduction of Atrial Fibrillation (STAR AF): a randomized, multicentre, international trial
Abstract
Aims: This multicentre, randomized trial compared three strategies of AF ablation: ablation of complex fractionated electrograms (CFE) alone, pulmonary vein isolation (PVI) alone, and combined PVI + CFE ablation, using standardized automated mapping software.
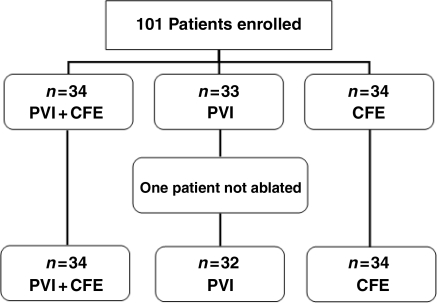
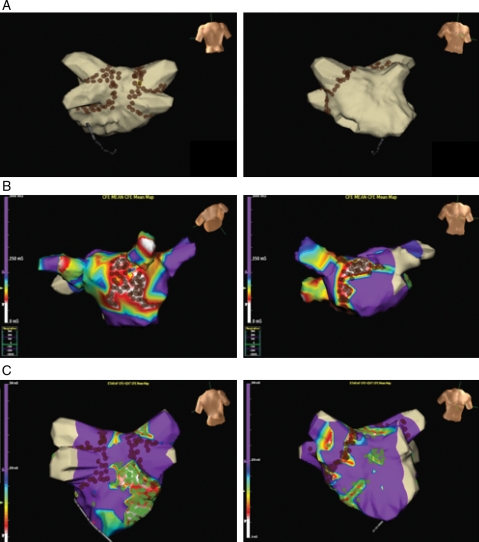
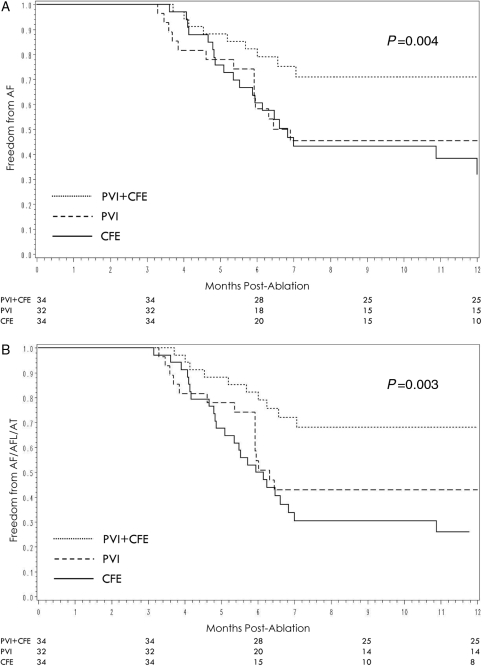
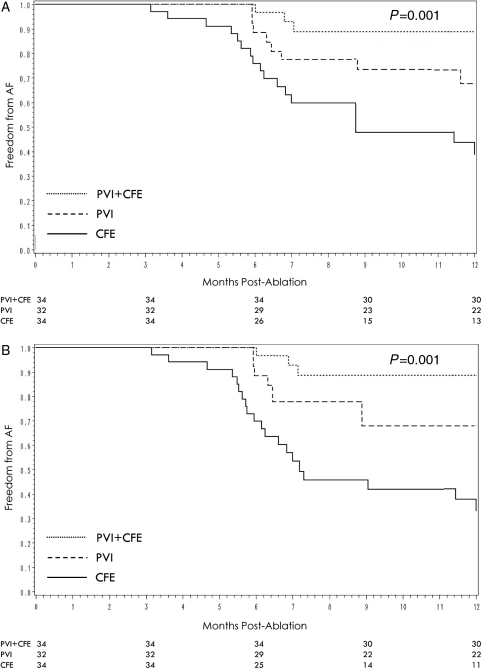
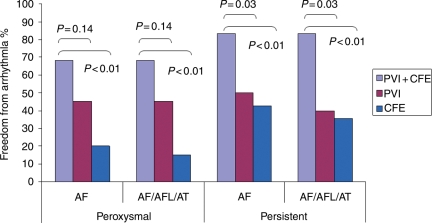
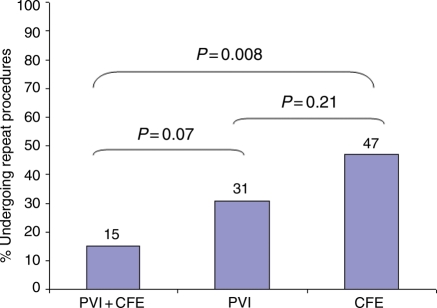
Methods and results: Patients with drug-refractory, high-burden paroxysmal (episodes >6 h, >4 in 6 months) or persistent atrial fibrillation (AF) were enrolled at eight centres. Patients (n = 100) were randomized to one of three arms. For CFE alone (n = 34), spontaneous/induced AF was mapped using validated, automated CFE software and all sites <120 ms were ablated until AF termination/non-inducibility. For PVI (n = 32), all four PV antra were isolated and confirmed using a circular catheter. For PVI + CFE (n = 34), all four PV antra were isolated, followed by AF induction and ablation of all CFE sites until AF termination/non-inducibility. Patients were followed at 3, 6, and 12 months with a visit, ECG, 48 h Holter. Atrial fibrillation symptoms were confirmed by loop recording. Repeat procedures were allowed within the first 6 months. The primary endpoint was freedom from AF >30 s at 1 year. Patients (age 57 +/- 10 years, LA size 42 +/- 6 mm) were 35% persistent AF. In CFE, ablation terminated AF in 68%. Only 0.4 PVs per patient were isolated as a result of CFE. In PVI, 94% had all four PVs successfully isolated. In PVI + CFE, 94% had all four PVs isolated, 76% had inducible AF with additional CFE ablation, with 73% termination of AF. There were significantly more repeat procedures in the CFE arm (47%) vs. PVI (31%) or PVI + CFE (15%) (P = 0.01). After one procedure, PVI + CFE had a significantly higher freedom from AF (74%) compared with PVI (48%) and CFE (29%) (P = 0.004). After two procedures, PVI + CFE still had the highest success (88%) compared with PVI (68%) and CFE (38%) (P = 0.001). Ninety-six percent of these patients were off anti-arrhythmics. Complications were two tamponades, no PV stenosis, and no mortality.
Conclusion: In high-burden paroxysmal/persistent AF, PVI + CFE has the highest freedom from AF vs. PVI or CFE alone after one or two procedures. Complex fractionated electrogram alone has the lowest one and two procedure success rates with a higher incidence of repeat procedures. ClinicalTrials.gov identifier number NCT00367757.
Figures
References
-
- Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijns HJ, Damiano RJ, Jr, Davies DW, Haines DE, Haissaguerre M, Iesaka Y, Jackman W, Jais P, Kottkamp H, Kuck KH, Lindsay BD, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Natale A, Pappone C, Prystowsky E, Raviele A, Ruskin JN, Shemin RJ. HRS/EHRA/ECAS expert Consensus Statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up. A report of the Heart Rhythm Society (HRS) Task Force on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2007;4:816–861. - PubMed
-
- Verma A, Kilicaslan F, Pisano E, Marrouche NF, Fanelli R, Brachmann J, Geunther J, Potenza D, Martin DO, Cummings J, Burkhardt JD, Saliba W, Schweikert RA, Natale A. Response of atrial fibrillation to pulmonary vein antrum isolation is directly related to resumption and delay of pulmonary vein conduction. Circulation. 2005;112:627–635. - PubMed
-
- Konings KT, Smeets JL, Penn OC, Wellens HJ, Allessie MA. Configuration of unipolar atrial electrograms during electrically induced atrial fibrillation in humans. Circulation. 1997;95:1231–1241. - PubMed
-
- Nademanee K, McKenzie J, Kosar E, Schwab M, Sunsaneewitayakul B, Vasavakul T, Khunnawat C, Ngarmukos T. A new approach for catheter ablation of atrial fibrillation: mapping of the electrophysiologic substrate. J Am Coll Cardiol. 2004;43:2044–2053. - PubMed
-
- Oral H, Chugh A, Good E, Wimmer A, Dey S, Gadeela N, Sankaran S, Crawford T, Sarrazin JF, Kuhne M, Chalfoun N, Wells D, Frederick M, Fortino J, Benloucif-Moore S, Jongnarangsin K, Pelosi F, Jr, Bogun F, Morady F. Radiofrequency catheter ablation of chronic atrial fibrillation guided by complex electrograms. Circulation. 2007;115:2606–2612. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
