

Effects of cardiac autonomic dysfunction on mortality risk in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial
- PMID: 20215456
- PMCID: PMC2890362
- DOI: 10.2337/dc10-0125
Effects of cardiac autonomic dysfunction on mortality risk in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial
Abstract
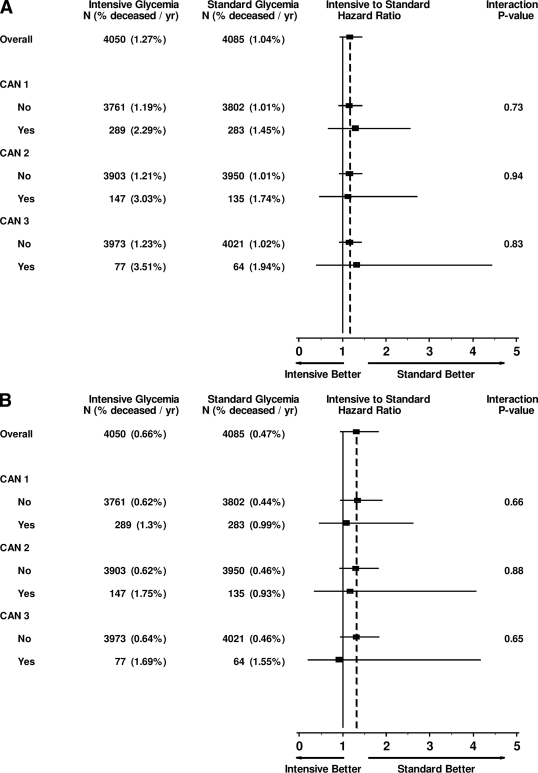
Objective: Intensive therapy targeting normal blood glucose increased mortality compared with standard treatment in a randomized clinical trial of 10,251 participants with type 2 diabetes at high-risk for cardiovascular disease (CVD) events. We evaluated whether the presence of cardiac autonomic neuropathy (CAN) at baseline modified the effect of intensive compared with standard glycemia treatment on mortality outcomes in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial participants.
Research design and methods: CAN was assessed by measures of heart rate variability (HRV) and QT index (QTI) computed from 10-s resting electrocardiograms in 8,135 ACCORD trial participants with valid measurements (mean age 63.0 years, 40% women). Prespecified CAN definitions included a composite of the lowest quartile of HRV and highest QTI quartile in the presence or absence of peripheral neuropathy. Outcomes were all-cause and CVD mortality. Associations between CAN and mortality were evaluated by proportional hazards analysis, adjusting for treatment group allocation, CVD history, and multiple prespecified baseline covariates.
Results: During a mean 3.5 years follow-up, there were 329 deaths from all causes. In fully adjusted analyses, participants with baseline CAN were 1.55-2.14 times as likely to die as participants without CAN, depending on the CAN definition used (P < 0.02 for all). The effect of allocation to the intensive group on all-cause and CVD mortality was similar in participants with or without CAN at baseline (P(interaction) > 0.7).
Conclusions: Whereas CAN was associated with increased mortality in this high-risk type 2 diabetes cohort, these analyses indicate that participants with CAN at baseline had similar mortality outcomes from intensive compared with standard glycemia treatment in the ACCORD cohort.
Trial registration: ClinicalTrials.gov NCT00000620.
Figures
Comment in
-
Neuropathy: the crystal ball for cardiovascular disease?Diabetes Care. 2010 Jul;33(7):1688-90. doi: 10.2337/dc10-0745. Diabetes Care. 2010. PMID: 20587730 Free PMC article. No abstract available.
References
-
- The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. The Diabetes Control and Complications Trial Research Group N Engl J Med 1993; 329: 977–986 - PubMed
-
- Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). UK Prospective Diabetes Study (UKPDS) Group. Lancet 1998; 352: 837–853 - PubMed
-
- Young LH, Wackers FJ, Chyun DA, Davey JA, Barrett EJ, Taillefer R, Heller GV, Iskandrian AE, Wittlin SD, Filipchuk N, Ratner RE, Inzucchi SE: Cardiac outcomes after screening for asymptomatic coronary artery disease in patients with type 2 diabetes: the DIAD study: a randomized controlled trial. JAMA 2009; 301: 1547–1555 - PMC - PubMed
-
- Maser RE, Mitchell BD, Vinik AI, Freeman R: The association between cardiovascular autonomic neuropathy and mortality in individuals with diabetes: a meta-analysis. Diabetes Care 2003; 26: 1895–1901 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- N01 HC095179/HL/NHLBI NIH HHS/United States
- N01 HC095184/HL/NHLBI NIH HHS/United States
- N01-HC-95180/HC/NHLBI NIH HHS/United States
- N01 HC095178/HL/NHLBI NIH HHS/United States
- N01-HC-95184/HC/NHLBI NIH HHS/United States
- IAA-Y1-HC-1010/HC/NHLBI NIH HHS/United States
- N01 HC095182/HL/NHLBI NIH HHS/United States
- N01-HC-95183/HC/NHLBI NIH HHS/United States
- N01-HC-95178/HC/NHLBI NIH HHS/United States
- N01-HC-95179/HC/NHLBI NIH HHS/United States
- N01-HC-95181/HC/NHLBI NIH HHS/United States
- IAA-Y1-HC-9035/HC/NHLBI NIH HHS/United States
- N01 HC095180/HL/NHLBI NIH HHS/United States
- Y01 HC001010/HC/NHLBI NIH HHS/United States
- Y01 HC009035/HC/NHLBI NIH HHS/United States
- N01 HC095181/HL/NHLBI NIH HHS/United States
- N01-HC-95182/HC/NHLBI NIH HHS/United States
- N01 HC095183/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
