

Size, shape, and stamina: the impact of left ventricular geometry on exercise capacity
- PMID: 20215563
- PMCID: PMC2856936
- DOI: 10.1161/HYPERTENSIONAHA.109.146845
Size, shape, and stamina: the impact of left ventricular geometry on exercise capacity
Abstract
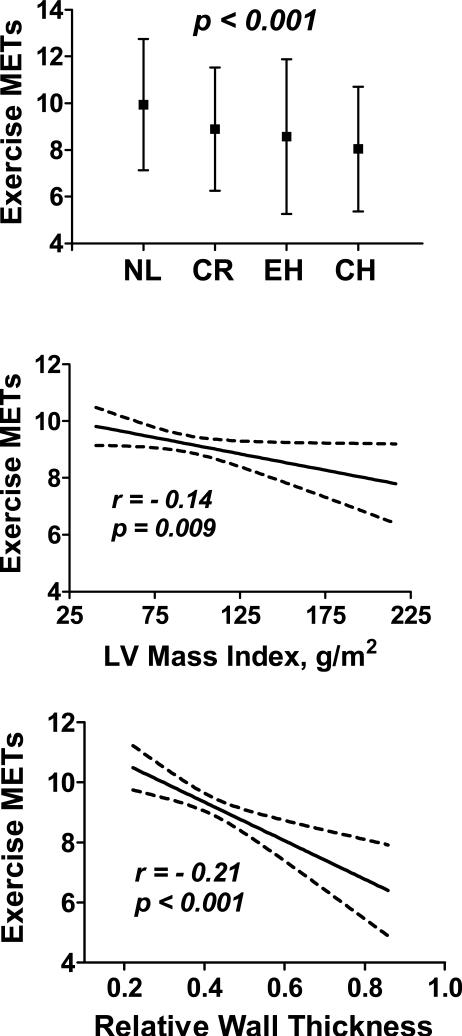
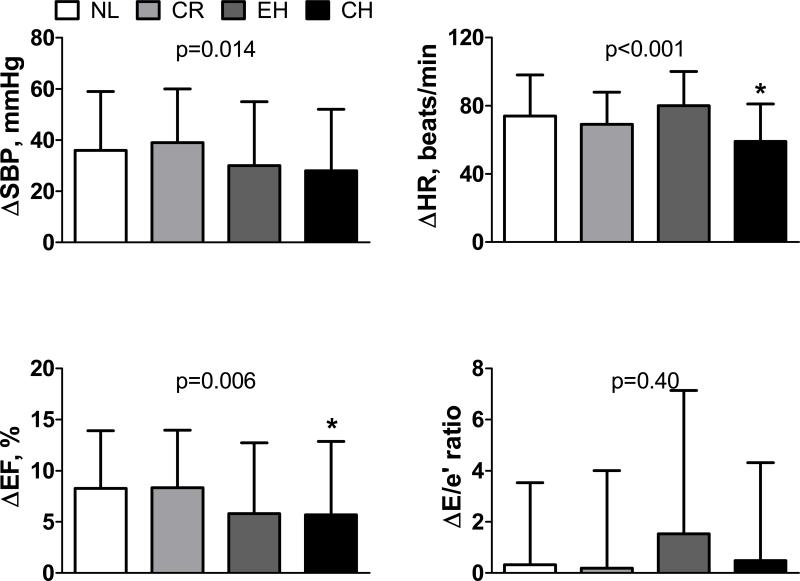
Although several studies have examined the cardiac functional determinants of exercise capacity, few have investigated the effects of structural remodeling. The current study evaluated the association between cardiac geometry and exercise capacity. Subjects with ejection fraction > or = 50% and no valvular disease, myocardial ischemia, or arrhythmias were identified from a large prospective exercise echocardiography database. Left ventricular mass index and relative wall thickness were used to classify geometry into normal, concentric remodeling, eccentric hypertrophy, and concentric hypertrophy. All of the subjects underwent symptom-limited treadmill exercise according to standard Bruce protocol. Maximal exercise tolerance was measured in metabolic equivalents. Of 366 (60+/-14 years; 57% male) subjects, 166 (45%) had normal geometry, 106 (29%) had concentric remodeling, 40 (11%) had eccentric hypertrophy, and 54 (15%) had concentric hypertrophy. Geometry was related to exercise capacity: in descending order, the maximum achieved metabolic equivalents were 9.9+/-2.8 in normal, 8.9+/-2.6 in concentric remodeling, 8.6+/-3.1 in eccentric hypertrophy, and 8.0+/-2.7 in concentric hypertrophy (all P<0.02 versus normal). Left ventricular mass index and relative wall thickness were negatively correlated with exercise tolerance in metabolic equivalents (r=-0.14; P=0.009 and r=-0.21; P<0.001, respectively). Augmentation of heart rate and ejection fraction with exercise were blunted in concentric hypertrophy compared with normal, even after adjusting for medications. In conclusion, the pattern of ventricular remodeling is related to exercise capacity among low-risk adults. Subjects with concentric hypertrophy display the greatest limitation, and this is related to reduced systolic and chronotropic reserve. Reverse remodeling strategies may prevent or treat functional decline in patients with structural heart disease.
Figures
References
-
- Najjar SS, Schulman SP, Gerstenblith G, Fleg JL, Kass DA, O'Connor F, Becker LC, Lakatta EG. Age and gender affect ventricular-vascular coupling during aerobic exercise. J Am Coll Cardiol. 2004;44:611–617. - PubMed
-
- Park S, Ha JW, Shim CY, Choi EY, Kim JM, Ahn JA, Lee SW, Rim SJ, Chung N. Gender-related difference in arterial elastance during exercise in patients with hypertension. Hypertension. 2008;51:1163–1169. - PubMed
-
- Chantler PD, Melenovsky V, Schulman SP, Gerstenblith G, Becker LC, Ferrucci L, Fleg JL, Lakatta EG, Najjar SS. The sex-specific impact of systolic hypertension and systolic blood pressure on arterial-ventricular coupling at rest and during exercise. Am J Physiol Heart Circ Physiol. 2008;295:H145–153. - PMC - PubMed
-
- Borlaug BA, Melenovsky V, Russell SD, Kessler K, Pacak K, Becker LC, Kass DA. Impaired chronotropic and vasodilator reserves limit exercise capacity in patients with heart failure and a preserved ejection fraction. Circulation. 2006;114:2138–2147. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
