

Predicting cardiac rehabilitation attendance in a gender-tailored randomized clinical trial
- PMID: 20216324
- PMCID: PMC2913420
- DOI: 10.1097/HCR.0b013e3181d0c2ce
Predicting cardiac rehabilitation attendance in a gender-tailored randomized clinical trial
Abstract
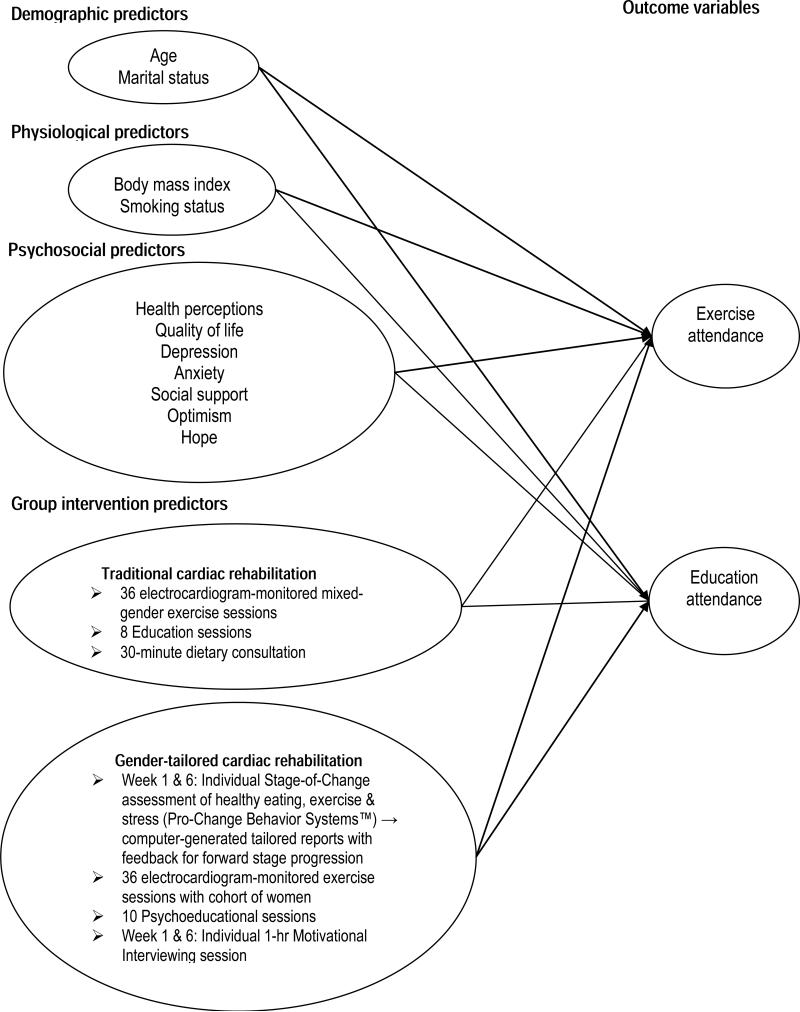
Purpose: This study compared attendance of women participating in a motivationally enhanced, gender-tailored cardiac rehabilitation (CR) program with that of women attending a traditional outpatient CR program. We also sought to determine the significant baseline predictors of attendance of the exercise and education components of the interventions.
Methods: Data from 252 women with CHD in the randomized clinical trial, the Women's-Only Cardiac Rehabilitation Program, were used in this study. The experimental design used 2 treatment groups: both receiving a comprehensive, 12-week, CR program, with 1 group receiving a gender-tailored, stage-of-change matched, behavioral enhancement using individualized motivational interviewing.
Results: Compared with women in the traditional CR program, women in the gender-tailored program attended significantly more of the prescribed exercise (90% vs 77%) and education sessions (87% vs 56%). Group assignment accounted for about 5% of the variance in exercise attendance (F1,250 = 12.755, P < .001) and about 24% of the variance in education attendance (F1,250 = 77.942, P < .001). After controlling for group assignment, the baseline characteristics of smoking status, marital status, and anxiety accounted for about 17% of the variance in exercise attendance (F5,245 = 10.494, P < .001). Smoking status and marital status were significant baseline predictors of education attendance (F5,245 = 6.115, P < .001) after controlling for group assignment.
Conclusions: The long-standing, poor attendance of women in CR continues to be an unresolved international challenge. Gender-tailored, stage-matched, CR programs hold promise for enhancing attendance to prescribed protocols. Additional research examining the efficacy of gender-sensitive, motivationally enhanced CR for women compared with generic CR programs is warranted.
Figures

References
-
- Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics--2009 Update. A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:e21–181. - PubMed
-
- Jneid H, Fonarow GC, Cannon CP, et al. Sex differences in medical care and early death after acute myocardial infarction. Circulation. 2008;118:2803–2810. - PubMed
-
- Wenger NK. Current status of cardiac rehabilitation. J Am Coll Cardiol. 2008;51:1619–1631. - PubMed
-
- Thomas RJ, King M, Lui K, et al. AACVPR/ACC/AHA 2007 performance measures on cardiac rehabilitation for referral to and delivery of cardiac rehabilitation/secondary prevention services endorsed by the American College of Chest Physicians, American College of Sports Medicine, American Physical Therapy Association, Canadian Association of Cardiac Rehabilitation, European Association for Cardiovascular Prevention and Rehabilitation, Inter-American Heart Foundation, National Association of Clinical Nurse Specialists, Preventive Cardiovascular Nurses Association, and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2007;50:1400–1433. - PubMed
-
- Smith SC, Jr., Allen J, Blair SN, et al. AHA/ACC guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 update: endorsed by the National Heart, Lung, and Blood Institute. Circulation. 2006;113:2363–2372. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
