

Review
doi: 10.1007/s00256-010-0909-1.
Epub 2010 Mar 10.
A systematised MRI approach to evaluating the patellofemoral joint
Affiliations
- PMID: 20217407
- PMCID: PMC2919651
- DOI: 10.1007/s00256-010-0909-1
Item in Clipboard
Review
A systematised MRI approach to evaluating the patellofemoral joint
Skeletal Radiol.
2011 Apr.
Abstract
Knee pain in young patients is a common indication for knee MRI. Many static and dynamic internal derangements of the patellofemoral joint in these patients lead to various secondary MRI findings. This article focuses on how to systematically approach, detect, and emphasize the importance of these findings in the diagnosis of patellofemoral tracking and impingement syndromes with relevant case examples.
Figures
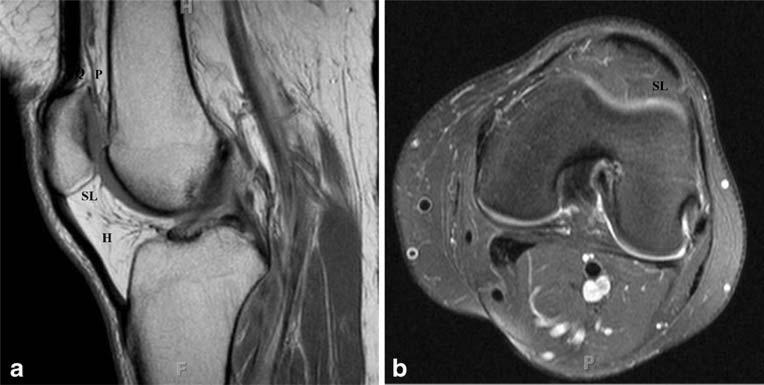
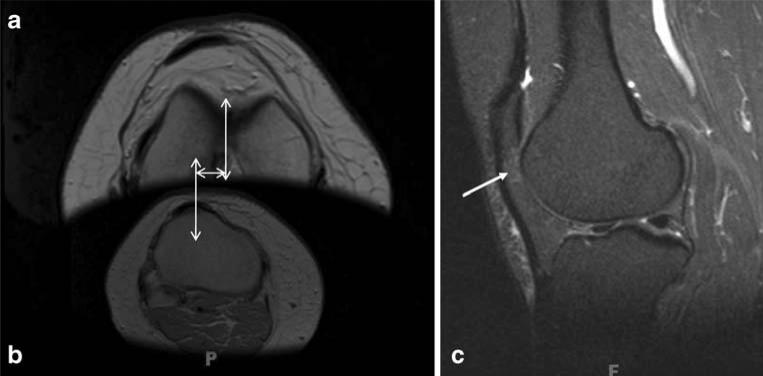
a Sagittal proton density-weighted (PDW) and b axial T2-weighted fat-saturated (T2Wfs) images demonstrate a normal quadriceps fat pad (Q), a prefemoral fat pad (P), Hoffa's fat pad (H), and a superolateral Hoffa's fat pad (SL)

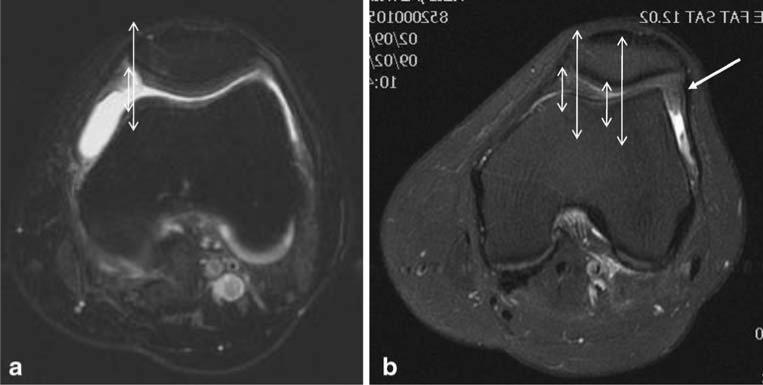
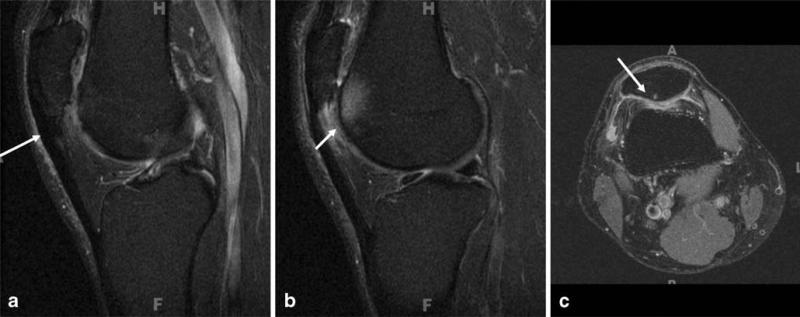
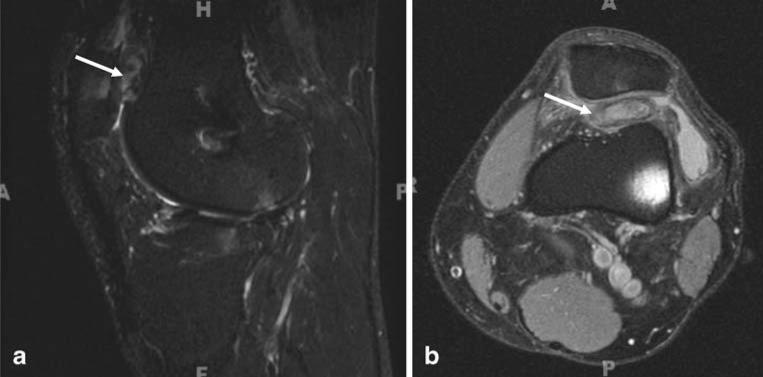
A 25-year-old woman with anterolateral knee pain. a Sagittal T2Wfs and b axial T2Wfs images demonstrate superolateral Hoffa's fat pad edema (large arrows). Also notice the hypertrophy of the SL fat pad extending far beyond the lateral retinaculum and causing anterior bowing of the patellar tendon (small arrows)
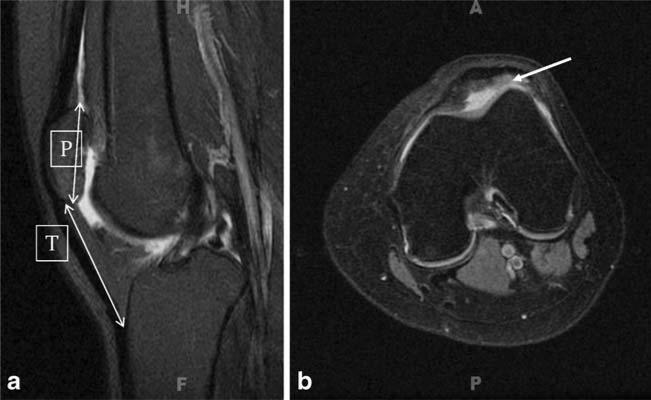
a Sagittal T2fs and b axial T2Wfs images showing an abnormal Insall–Salvati ratio of 1.5 (patellar length [P] to patellar tendon [T] ratio) in a 19-year-old woman with anterolateral knee pain. Notice superolateral Hoffa's fat pad edema (arrow) on the axial T2Wfs (b)
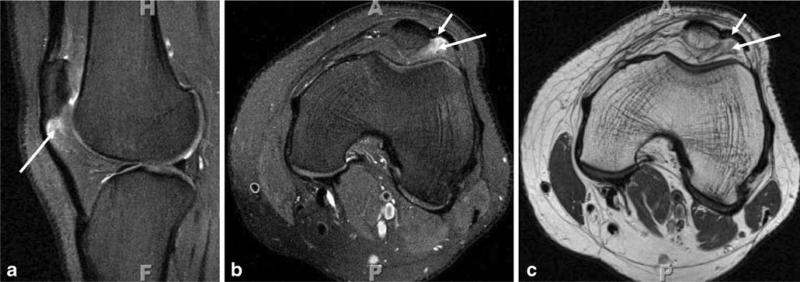
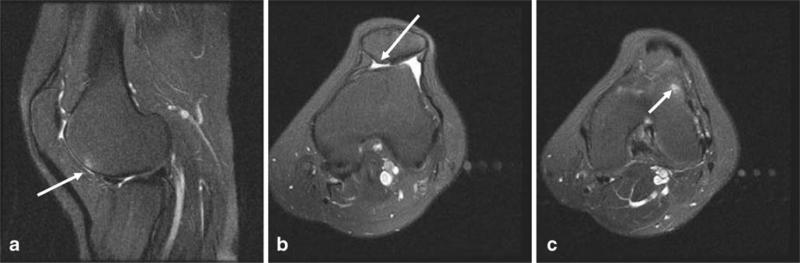
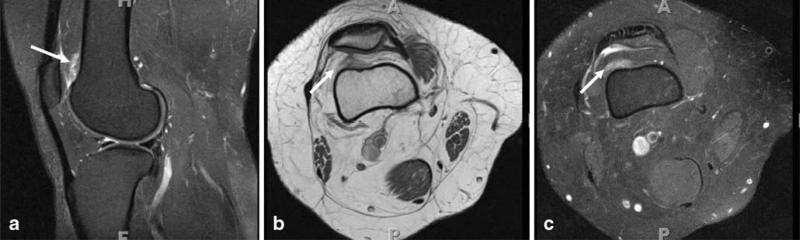
a Sagittal T2Wfs, b axial T2Wfs, and c axial PDW images in another case of patella alta with superolateral Hoffa's fat pad edema (long arrows). Notice Hoffa's fat pad enlargement with abnormal bowing of the patellar tendon (small arrows)
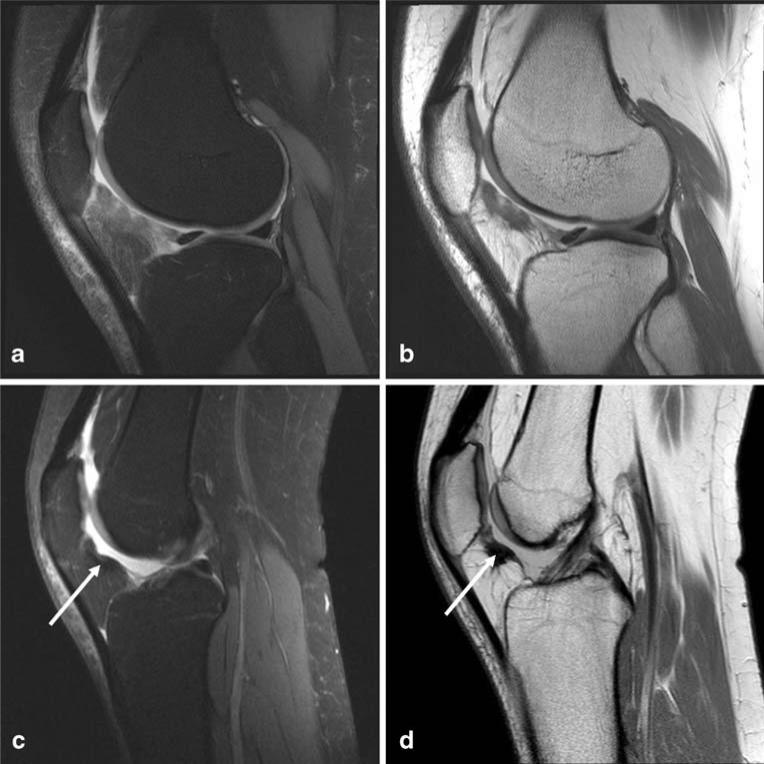
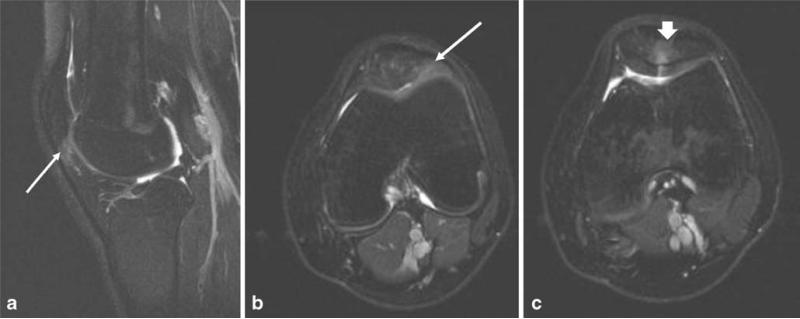
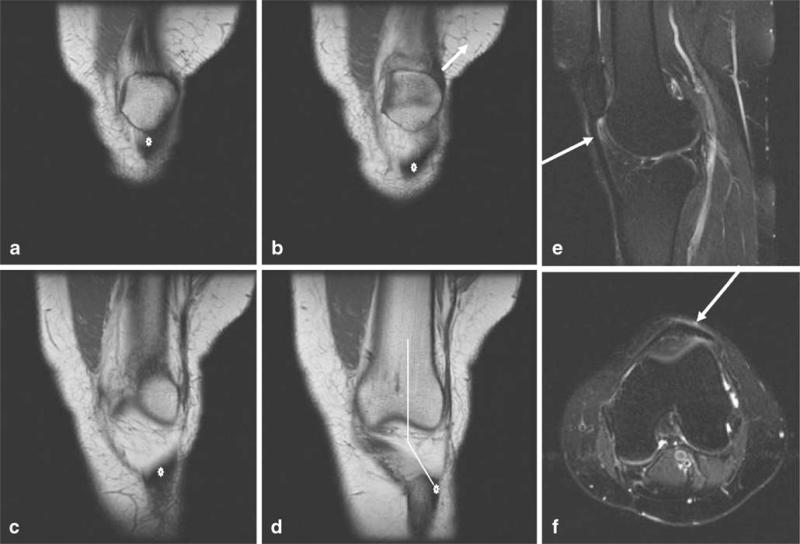
Traumatic Hoffitis in a 27-year-old woman with a history of a motor vehicle accident. a Initial sagittal PDWfs and b sagittal PDW images 2 years before at the time of the insult demonstrate a shearing injury to Hoffa's fat pad with diffuse edema and irregular contour. c, d Persistent anterior knee pain led to another MRI, which demonstrated posterior superior Hoffa's fat pad fibrosis (arrows) as focal hypointensity on sagittal PDWfs (c) and sagittal PDW (d) images. No other internal derangement was identified
a Normal patellar location with patellar apex congruent to femoral trochlear sulcus and less than 2 mm distance between lines drawn along the medial patellar facet (short line) and medial femoral trochlea (longer line; axial T2Wfs image). b Another patient with abnormal lateral patellar translation (axial T2Wfs image). Also notice superolateral Hoffa's fat pad hypertrophy extending below the lateral retinaculum (arrow)
A 27-year-old man with anterolateral knee pain walking upstairs. a Sagittal T2Wfs and b, c axial T2Wfs images demonstrate superolateral Hoffa's fat pad edema (long arrows). Notice abnormal patellar tilt (c) with relatively decreased lateral patellofemoral joint space, and the patellofemoral angle measured 5°. Also note the full thickness chondral fissure at the median ridge with subchondral edema (thick arrow)
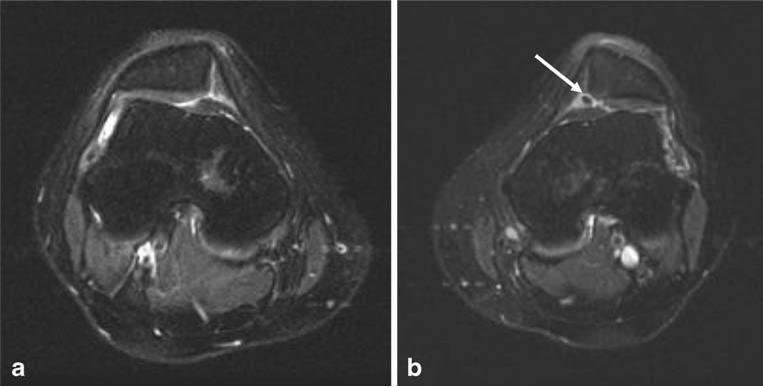
A 20-year-old woman with bilateral anterolateral knee pain. a, b Axial T2Wfs images of both knees demonstrate findings of excessive lateral pressure syndrome (ELPS) and abnormal lateral patellar tilt without lateral translation. There was bilateral superolateral Hoffa's fat pad edema (not shown). Also note the underlying trochlear sulcus hypoplasia and loose cartilaginous body from the median ridge of the left patella (arrow)
Axial T2Wfs images. a Normal trochlear sulcus (sulcus angle measuring <144°). b Hypoplastic sulcus (sulcus angle measuring = 168°) and c dysplastic sulcus (absent sulcus with abnormal trochlear convexity)
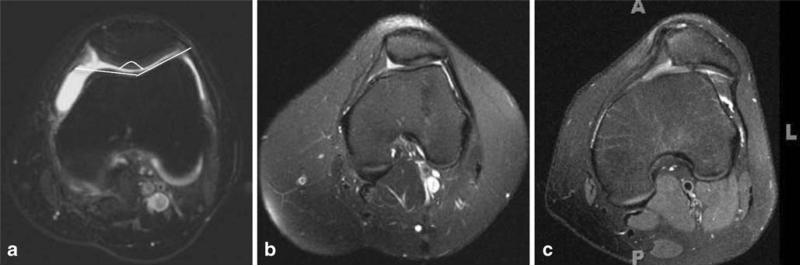
A 43-year-old woman with excessive lateral friction syndrome (ELFS). a, b Notice increased TT–TG distance measuring 2.3 cm depicted on sequential axial PDW images superimposed on each other. c Also note the subtle superolateral Hoffa's fat pad edema on a sagittal T2Wfs image (arrow)
A 36-year-old woman with excessive lateral friction syndrome (ELFS) due to lateralized patellar tendon (marker) depicted on a–d sequential coronal T1W images with an abnormal Q angle equivalent (d). Notice e superolateral Hoffa's fat pad edema on the sagittal T2Wfs image (arrow) and f the abnormally located patellar tendon on axial T2Wfs image (arrow)
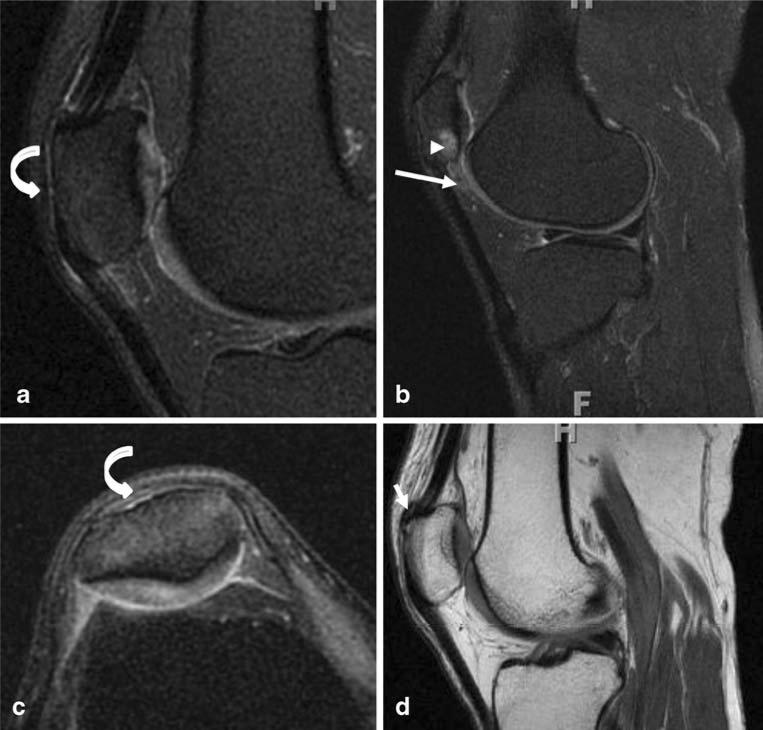
A 50-year-old woman who had suffered from nontraumatic anterior knee pain for many months. a, b Sagittal PDWfs, c axial PDWfs and d sagittal PDW images show acute partial quadriceps tendon stripping of the anterior patella (curved arrows in a,c), superolateral Hoffa's fat pad edema (long arrow in b), and subchondral edema of the lateral facet of the patella related to chondrosis (arrowhead in b). There is underlying trochlear sulcus hypoplasia (c). d Also note the chronic enthesopathic change in the superior patella (short arrow)
An 18-year-old boy with persistent knee pain, status post-medial retinacular repair. a, c Sagittal PDWfs and b, d axial PDWfs images show susceptibility artifacts from the surgery (arrow in a), persistent lateral subluxation and tilt of the patella and trochlear sulcus dysplasia (b), patella alta with subtle superolateral Hoffa's fat pad edema (arrow in c). There is partial re-tearing of the patellar insertion of the medial retinaculum (arrow in d) and median ridge patellar chondrosis
A 35-year-old man with chronic jumper's knee. a, b Sagittal PDWfs and c axial PDWfs images show focally thickened proximal patellar tendon (arrow in a). Notice superolateral Hoffa's fat pad edema as well as lateral trochlear (arrow in b) and lateral facet patellar chondrosis with subchondral cystic change and edema (arrow in c)

A 35-year-old man with Osgood–Schlatter disease. a Sagittal PDW and b, c axial PDWfs images show a thickened distal patellar tendon (arrow in a). Notice lateral facet patellar chondrosis (arrow in b) and superolateral Hoffa's fat pad edema (arrow in c)
A 30-year-old woman with anterior knee pain. a Sagittal T2Wfs and b, c axial T2Wfs images show patella alta (a), dysplastic sulcus (b), and laterally transposed patellar tendon in keeping with excessive lateral friction syndrome (ELFS; c). Notice secondary patellofemoral osteoarthritis (arrows)
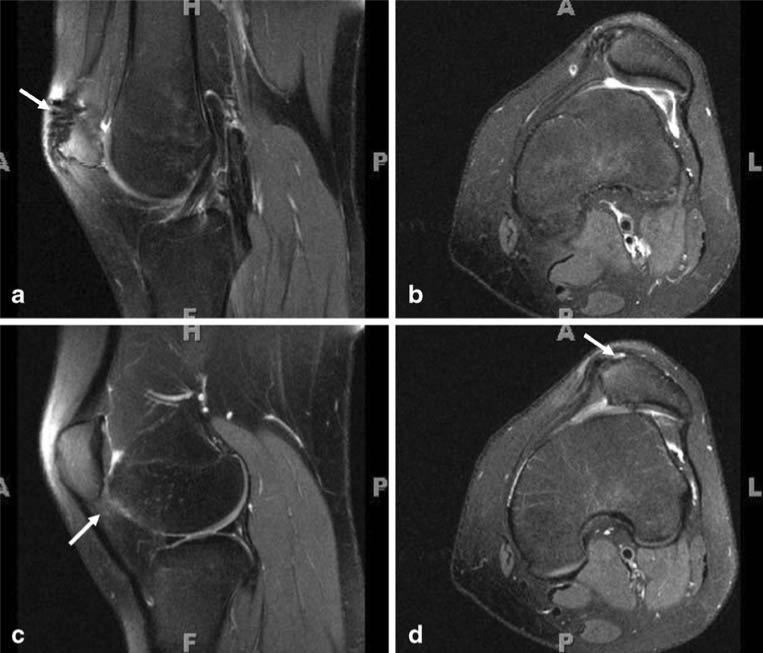
A 48-year-old man with long-standing anterior knee pain. a Sagittal T2Wfs, b axial T2Wfs, c coronal T1W, and d coronal T2Wfs images demonstrate synovitis and early adventitial bursa formation of the superior Hoffa's fat pad (arrows in a, c, d). Notice the underlying shallow trochlear sulcus and abnormal patellar tilt with secondary patellar chondrosis (short arrow in b)
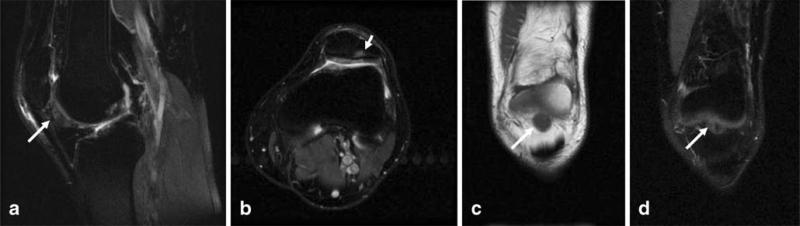
a Sagittal PDWfs and b PDW images. The infrapatellar fat pad is one of the most common locations for a ganglion cyst of the knee (arrows). This should not be confused with adventitial bursa formation due to Hoffa's fat pad impingement
A young girl with anterior knee pain. a Sagittal PDWfs, b axial PDW, and c axial PDWfs images show patella alta (a) and isolated prefemoral fat pad edema related to impingement (arrows)
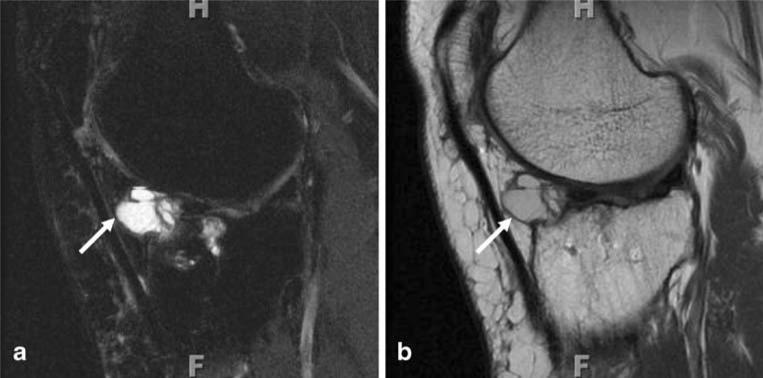
A 42-year-old man s/p anterior cruciate ligament graft with persistent knee pain. The graft was intact. a Sagittal PDWfs and b axial PDWfs images show impingement-related adventitial bursa formation of the prefemoral fat pad (arrows). Minimal patella alta (Insall–Salvati ratio 1.3) was also present
References
-
- Hungerford DS, Barry M. Biomechanics of the patellofemoral joint. Clin Orthop Relat Res. 1979;(144):9–15. - PubMed
-
- Faber SC, Eckstein F, Lukasz S, et al. Gender differences in knee joint cartilage thickness, volume and articular surface areas: assessment with quantitative three-dimensional MR imaging. Skeletal Radiol. 2001;30:144–50. - PubMed
-
- Fucentese SF, von Roll A, Koch PP, Epari DR, Fuchs B, Schottle PB. The patella morphology in trochlear dysplasia—a comparative MRI study. Knee. 2006;13:145–50. - PubMed
-
- Tecklenburg K, Dejour D, Hoser C, Fink C. Bony and cartilaginous anatomy of the patellofemoral joint. Knee Surg Sports Traumatol Arthrosc. 2006;14:235–40. - PubMed
-
- McNally EG, Ostlere SJ, Pal C, Phillips A, Reid H, Dodd C. Assessment of patellar maltracking using combined static and dynamic MRI. Eur Radiol. 2000;10:1051–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
