

Small bowel obstruction-who needs an operation? A multivariate prediction model
- PMID: 20217412
- PMCID: PMC4882094
- DOI: 10.1007/s00268-010-0479-3
Small bowel obstruction-who needs an operation? A multivariate prediction model
Abstract
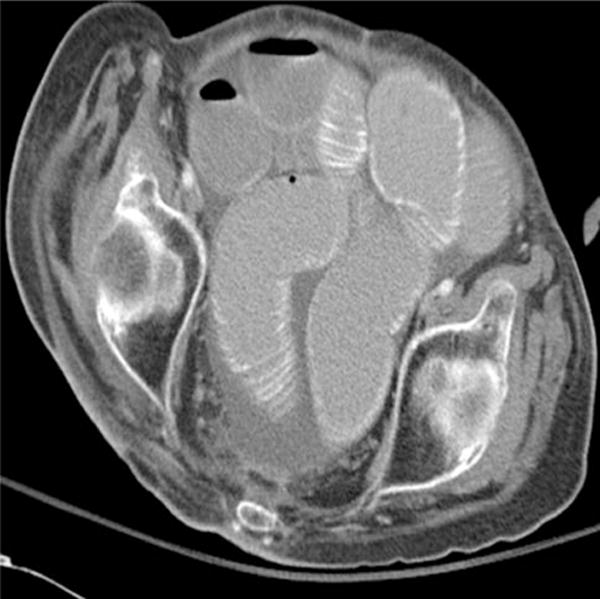
Background: Proper management of small bowel obstruction (SBO) requires a methodology to prevent nontherapeutic laparotomy while minimizing the chance of overlooking strangulation obstruction causing intestinal ischemia. Our aim was to identify preoperative risk factors associated with strangulating SBO and to develop a model to predict the need for operative intervention in the presence of an SBO. Our hypothesis was that free intraperitoneal fluid on computed tomography (CT) is associated with the presence of bowel ischemia and need for exploration.
Methods: We reviewed 100 consecutive patients with SBO, all of whom had undergone CT that was reviewed by a radiologist blinded to outcome. The need for operative management was confirmed retrospectively by four surgeons based on operative findings and the patient's clinical course.
Results: Patients were divided into two groups: group 1, who required operative management on retrospective review, and group 2 who did not. Four patients who were treated nonoperatively had ischemia or died of malignant SBO and were then included in group 1; two patients who had a nontherapeutic exploration were included in group 2. On univariate analysis, the need for exploration (n = 48) was associated (p < 0.05) with a history of malignancy (29% vs. 12%), vomiting (85% vs. 63%), and CT findings of either free intraperitoneal fluid (67% vs. 31%), mesenteric edema (67% vs. 37%), mesenteric vascular engorgement (85% vs. 67%), small bowel wall thickening (44% vs. 25%) or absence of the "small bowel feces sign" (so-called fecalization) (10% vs. 29%). Ischemia (n = 11) was associated (p < 0.05 each) with peritonitis (36% vs. 1%), free intraperitoneal fluid (82% vs. 44%), serum lactate concentration (2.7 +/- 1.6 vs. 1.3 +/- 0.6 mmol/l), mesenteric edema (91% vs. 46%), closed loop obstruction (27% vs. 2%), pneumatosis intestinalis (18% vs. 0%), and portal venous gas (18% vs. 0%). On multivariate analysis, free intraperitoneal fluid [odds ratio (OR) 3.80, 95% confidence interval (CI) 1.5-9.9], mesenteric edema (OR 3.59, 95% CI 1.3-9.6), lack of the "small bowel feces sign" (OR 0.19, 95% CI 0.05-0.68), and a history of vomiting (OR 4.67, 95% CI 1.5-14.4) were independent predictors of the need for operative exploration (p < 0.05 each). The combination of vomiting, no "small bowel feces sign," free intraperitoneal fluid, and mesenteric edema had a sensitivity of 96%, and a positive predictive value of 90% (OR 16.4, 95% CI 3.6-75.4) for requiring exploration.
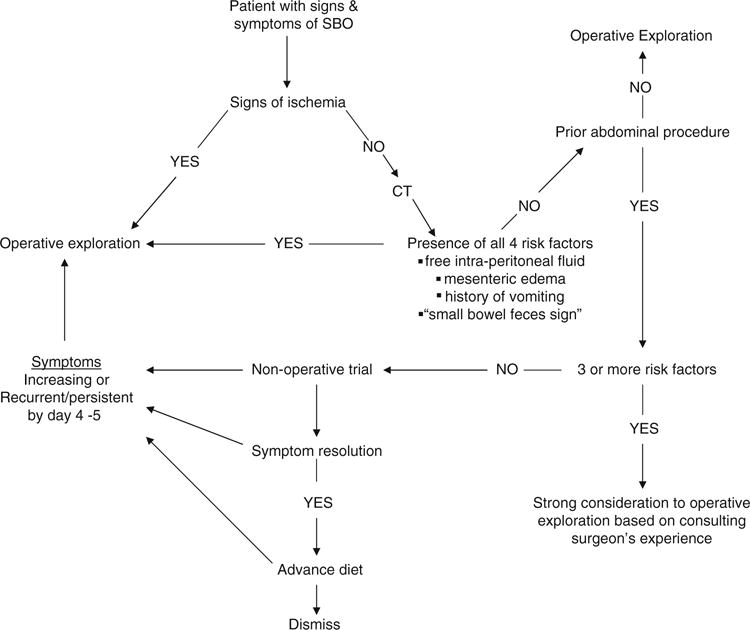
Conclusion: Clinical, laboratory, and radiographic factors should all be considered when making a decision about treatment of SBO. The four clinical features-intraperitoneal free fluid, mesenteric edema, lack of the "small bowel feces sign," history of vomiting-are predictive of requiring operative intervention during the patient's hospital stay and should be factored strongly into the decision-making algorithm for operative versus nonoperative treatment.
Figures

Comment in
-
Small bowel obstruction-who needs an operation?World J Surg. 2010 May;34(5):920-2. doi: 10.1007/s00268-010-0460-1. World J Surg. 2010. PMID: 20217413 No abstract available.
References
-
- Mucha P. Small intestinal obstruction. Surg Clin North Am. 1987;67:597–620. - PubMed
-
- Bizer LS, Liebling RW, Delany HM, et al. Small bowel obstruction. Surgery. 1981;89:407–413. - PubMed
-
- Silen W, Hein MF, Goldman L. Strangulation obstruction of the small intestine. Arch Surg. 1962;85:137–145. - PubMed
-
- Laws HL, Aldrete JS. Small bowel obstruction: a review of 465 cases. South Med J. 1976;69:733–734. - PubMed
-
- Bickell NA, Federman AD, Aufses AH. Influence of time on risk of bowel resection in complete small bowel obstruction. J Am Coll Surg. 2005;201:847–854. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
