

Adaptive radiation therapy for prostate cancer
- PMID: 20219551
- PMCID: PMC3664920
- DOI: 10.1016/j.semradonc.2009.11.007
Adaptive radiation therapy for prostate cancer
Abstract
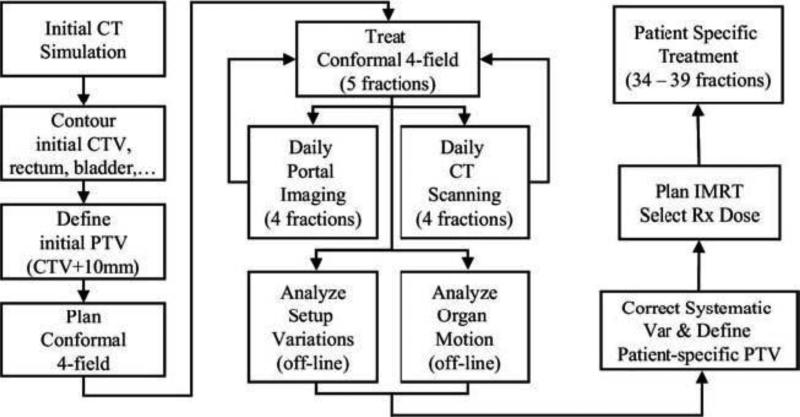
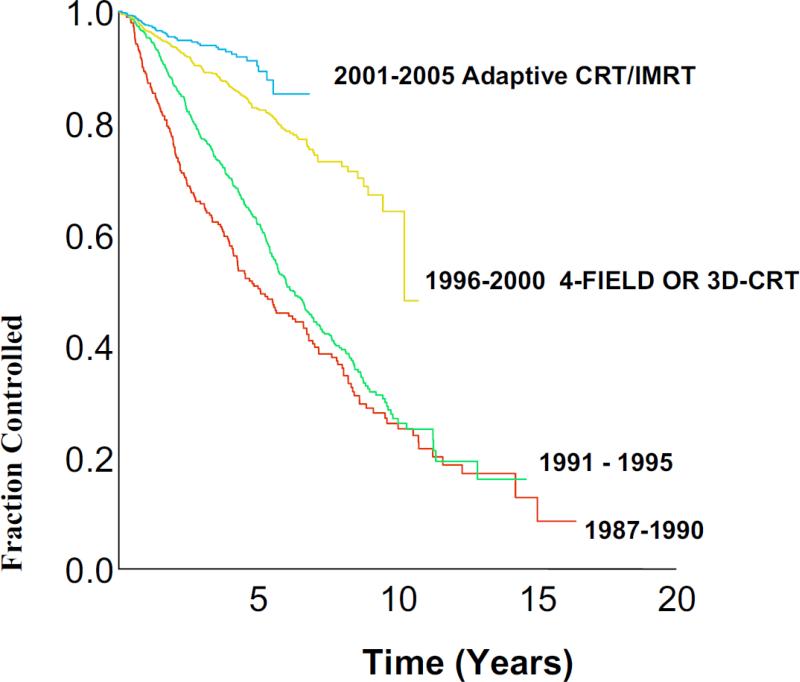
Adaptive radiotherapy has been introduced to manage an individual's treatment by, including patient-specific treatment variation identified and quantified during the course of radiotherapy in the treatment planning and delivering optimization. Early studies have demonstrated that this technique could significantly improve the therapeutic ratio by safely reducing the large target margin that has to be used in conventional radiotherapy for prostate cancer treatment. Clinical application of off-line image-guided adaptive radiotherapy for prostate cancer has demonstrated encouraging clinical outcome. Long-term clinical follow-up has shown significant improvement in terms of tumor control and low toxicity profile, emphasizing the beneficial effect of image-guidance and adaptive treatment. Continuous development in adaptive radiotherapy has made possible additional increases in target dose by further reducing target margin when using online image-guided adaptive intensity-modulated radiation therapy. However, clinical implementation of new techniques should be explored cautiously and should include a comprehensive management strategy to address uncertainties in target definition and delineation in the preclinical implementation studies.
Copyright 2010 Elsevier Inc. All rights reserved.
Figures
References
-
- De Crevoisier R, Tucker SL, Dong L, et al. Increased risk of biochemical and local failure in patients with distended rectum on the planning CT for prostate cancer radiotherapy. Int J Radiat Oncol Biol Phys. 2005;62:965–973. - PubMed
-
- Heemsbergen WD, Hoogeman MS, Witte MG, et al. Increased risk of biochemical and clinical failure for prostate patients with a large rectum at radiotherapy planning: Results from the Dutch trial of 68 Gy versus 78 Gy. Int J Radiat Oncol Biol Phys. 2007;67:1418–1424. - PubMed
-
- Yan D, Vicini F, Wong J, et al. Adaptive radiation therapy. Phys Med Biol. 1997;42:123–132. - PubMed
-
- Valicenti RK, Michalski JM, Bosch WR, et al. Is weekly port filming adequate for verifying patient position in modern radiation therapy. Int J Radiat Oncol Biol Phys. 1994;30:431–438. - PubMed
-
- Hunt MA, Schultheiss TE, Desobry GE. An evaluation of setup uncertainties for patients treated to pelvic sites. Int J Radiat Oncol Biol Phys. 1995;32:227–233. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
