

Determinants of renal disease variability in ADPKD
- PMID: 20219616
- PMCID: PMC2837603
- DOI: 10.1053/j.ackd.2009.12.004
Determinants of renal disease variability in ADPKD
Abstract
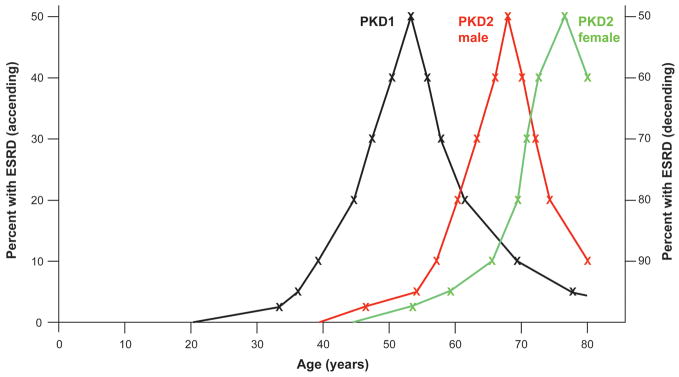
In common with other Mendelian diseases, the presentation and progression of autosomal dominant polycystic kidney disease (ADPKD) vary widely in the population. The typical course is of adult-onset disease with ESRD in the 6th decade. However, a small proportion has adequate renal function into the 9th decade, whereas others present with enlarged kidneys as neonates. ADPKD is genetically heterogeneous, and the disease gene is a major determinant of severity; PKD1 on average is associated with ESRD 20 years earlier than PKD2. The majority of PKD1 and PKD2 mutations are likely fully inactivating although recent studies indicate that some alleles retain partial activity (hypomorphic alleles). Homozygotes for such alleles are viable and in combination with an inactivating allele can result in early-onset disease. Hypomorphic alleles and mosaicism may also account for some cases with unusually mild disease. The degree of phenotypic variation detected in families indicates that genetic background influences disease severity. Genome-wide association studies are planned to map common variants associated with severity. Although ADPKD is a simple genetic disease, fully understanding the phenotypic variability requires consideration of influences at the genic, allelic, and genetic background level, and so, ultimately, it is complex.
2010 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no conflict of interest or financial disclosures significant to this article.
Figures
References
-
- OMIM(TM) Online Mendelian Inheritance in Man. McKusick-Nathans Institute of Genetic Medicine, Johns Hopkins University; Baltimore, MN: National Center for Biotechnology Information; Bethesda, MD: 2009.
-
- Klahr S, Breyer JA, Beck GJ, et al. Dietary protein restriction, blood pressure control, and the progression of polycystic kidney disease. Modification of Diet in Renal Disease Study Group. J Am Soc Nephrol. 1995;5:2037–2047. - PubMed
-
- Gabow PA, Johnson AM, Kaehny WD, et al. Factors affecting the progression of renal disease in autosomal-dominant polycystic kidney disease. Kidney Int. 1992;41:1311–1319. - PubMed
-
- Johnson AM, Gabow PA. Identification of pateints with autosomal dominant polycystic kidney disease at highest risk for end-stage renal disease. J Am Soc Nephrol. 1997:1560–1567. - PubMed
-
- Grantham JJ, Torres VE, Chapman AB, et al. Volume Progression in Polycystic Kidney Disease. N Engl J Med. 2006;354:2122–2130. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
