

Predictors of serum 25-hydroxyvitamin D concentrations among postmenopausal women: the Women's Health Initiative Calcium plus Vitamin D clinical trial
- PMID: 20219959
- PMCID: PMC2854906
- DOI: 10.3945/ajcn.2009.28908
Predictors of serum 25-hydroxyvitamin D concentrations among postmenopausal women: the Women's Health Initiative Calcium plus Vitamin D clinical trial
Abstract
Background: It is unclear how well surrogate markers for vitamin D exposure (eg, oral intake of vitamin D and estimates of sunlight exposure), with and without consideration of other potential predictors of 25-hydroxyvitamin D [25(OH)D] concentrations, similarly rank individuals with respect to 25(OH)D blood concentrations.
Objective: The objective was to determine how much variation in serum 25(OH)D concentrations (nmol/L) could be explained by a predictive model with the use of different vitamin D surrogate markers (latitude of residence, mean annual regional solar irradiance estimates, and oral sources) and other individual characteristics that might influence vitamin D status.
Design: A random sample of 3055 postmenopausal women (aged 50-70 y) participating in 3 nested case-control studies of the Women's Health Initiative Calcium plus Vitamin D Clinical Trial was used. Serum 25(OH)D values, assessed at year 1 (1995-2000), and potential predictors of 25(OH)D concentrations, assessed at year 1 or Women's Health Initiative baseline (1993-1998), were used.
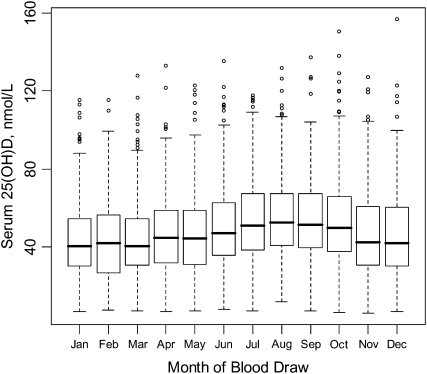
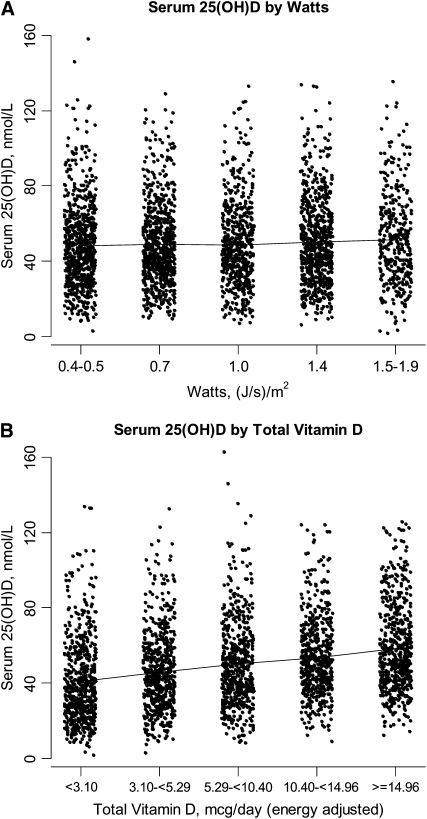
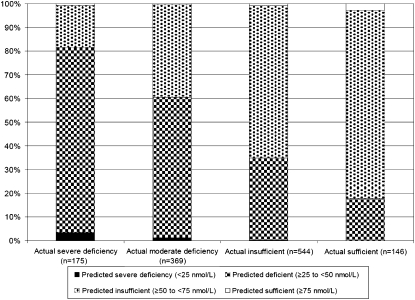
Results: More than half of the women (57.1%) had deficient (<50 nmol/L) concentrations of 25(OH)D. Distributions of 25(OH)D concentrations by level of latitude of residence, mean annual regional solar irradiance, and intake of vitamin D varied considerably. The predictive model for 25(OH)D explained 21% of the variation in 25(OH)D concentrations. After adjustment for month of blood draw, breast cancer status, colorectal cancer status, fracture status, participation in the hormone therapy trial, and randomization to the dietary modification trial, the predictive model included total vitamin D intake from foods and supplements, waist circumference, recreational physical activity, race-ethnicity, regional solar irradiance, and age.
Conclusions: Surrogate markers for 25(OH)D concentrations, although somewhat correlated, do not adequately reflect serum vitamin D measures. These markers and predictive models of blood 25(OH)D concentrations should not be given as much weight in epidemiologic studies of cancer risk.
Figures
Similar articles
-
Vitamin D intake determines vitamin d status of postmenopausal women, particularly those with limited sun exposure.J Nutr. 2014 May;144(5):681-9. doi: 10.3945/jn.113.183541. Epub 2014 Mar 5. J Nutr. 2014. PMID: 24598886 Free PMC article.
-
Vitamin D status in postmenopausal women living at higher latitudes in the UK in relation to bone health, overweight, sunlight exposure and dietary vitamin D.Bone. 2008 May;42(5):996-1003. doi: 10.1016/j.bone.2008.01.011. Epub 2008 Feb 9. Bone. 2008. PMID: 18329355
-
Serum 25-hydroxyvitamin D concentrations in relation to cardiometabolic risk factors and metabolic syndrome in postmenopausal women.Am J Clin Nutr. 2011 Jul;94(1):209-17. doi: 10.3945/ajcn.110.010272. Epub 2011 May 25. Am J Clin Nutr. 2011. PMID: 21613558 Free PMC article. Clinical Trial.
-
Relative importance of summer sun exposure, vitamin D intake, and genes to vitamin D status in Dutch older adults: The B-PROOF study.J Steroid Biochem Mol Biol. 2016 Nov;164:168-176. doi: 10.1016/j.jsbmb.2015.08.008. Epub 2015 Aug 11. J Steroid Biochem Mol Biol. 2016. PMID: 26275945 Review.
-
Vitamin D requirements: current and future.Am J Clin Nutr. 2004 Dec;80(6 Suppl):1735S-9S. doi: 10.1093/ajcn/80.6.1735S. Am J Clin Nutr. 2004. PMID: 15585797 Review.
Cited by
-
Gut microbiome dysregulation drives bone damage in broiler tibial dyschondroplasia by disrupting glucose homeostasis.NPJ Biofilms Microbiomes. 2023 Jan 3;9(1):1. doi: 10.1038/s41522-022-00360-6. NPJ Biofilms Microbiomes. 2023. PMID: 36596826 Free PMC article.
-
Vitamin D status and intake of lactating Inuit women living in the Canadian Arctic.Public Health Nutr. 2018 Aug;21(11):1988-1994. doi: 10.1017/S1368980017004189. Epub 2018 Feb 13. Public Health Nutr. 2018. PMID: 29433587 Free PMC article.
-
Serum 25-Hydroxyvitamin D Concentrations and Incidence of Age-Related Macular Degeneration: The Atherosclerosis Risk in Communities Study.Invest Ophthalmol Vis Sci. 2019 Apr 1;60(5):1362-1371. doi: 10.1167/iovs.18-25945. Invest Ophthalmol Vis Sci. 2019. PMID: 30934055 Free PMC article.
-
Sex-specific determinants of serum 25-hydroxyvitamin D3 concentrations in an elderly German cohort: a cross-sectional study.Nutr Metab (Lond). 2015 Jan 14;12:2. doi: 10.1186/1743-7075-12-2. eCollection 2015. Nutr Metab (Lond). 2015. PMID: 25745506 Free PMC article.
-
Predictors of 25-Hydroxyvitamin D Concentration Measured at Multiple Time Points in a Multiethnic Population.Am J Epidemiol. 2017 Nov 15;186(10):1180-1193. doi: 10.1093/aje/kwx180. Am J Epidemiol. 2017. PMID: 28549072 Free PMC article.
References
-
- Grant WB, Mohr SB. Ecological studies of ultraviolet B, vitamin D and cancer since 2000. Ann Epidemiol 2009;19:446–54 - PubMed
-
- Giovannucci E. The epidemiology of vitamin D and cancer incidence and mortality: a review (United States). Cancer Causes Control 2005;16:83–95 - PubMed
-
- Bertone-Johnson ER. Vitamin D and breast cancer. Ann Epidemiol 2009;19:462–7 - PubMed
-
- Giovannucci E. Strengths and limitations of current epidemiologic studies: vitamin D as a modifier of colon and prostate cancer risk. Nutr Rev 2007;65:S77–9 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 WH42115/WH/WHI NIH HHS/United States
- N01 WH32112/WH/WHI NIH HHS/United States
- N01WH22110/WH/WHI NIH HHS/United States
- N01 WH42125/WH/WHI NIH HHS/United States
- N01 WH32108/WH/WHI NIH HHS/United States
- N01 WH32102/WH/WHI NIH HHS/United States
- N01 WH32113/WH/WHI NIH HHS/United States
- N01 WH42110/WH/WHI NIH HHS/United States
- N01 WH42130/WH/WHI NIH HHS/United States
- N01 WH42124/WH/WHI NIH HHS/United States
- N01 WH32115/WH/WHI NIH HHS/United States
- N01 WH44221/WH/WHI NIH HHS/United States
- N01 WH32109/WH/WHI NIH HHS/United States
- N01 WH32106/WH/WHI NIH HHS/United States
- N01 WH42114/WH/WHI NIH HHS/United States
- N01 WH32101/WH/WHI NIH HHS/United States
- N01 WH42121/WH/WHI NIH HHS/United States
- N01 WH32119/WH/WHI NIH HHS/United States
- N01 WH42111/WH/WHI NIH HHS/United States
- N01 WH42132/WH/WHI NIH HHS/United States
- N01 WH42112/WH/WHI NIH HHS/United States
- N01 WH42120/WH/WHI NIH HHS/United States
- N01 WH42129/WH/WHI NIH HHS/United States
- N01 WH32118/WH/WHI NIH HHS/United States
- N01 WH42131/WH/WHI NIH HHS/United States
- N01 WH42119/WH/WHI NIH HHS/United States
- UL1 RR025755/RR/NCRR NIH HHS/United States
- N01 WH42108/WH/WHI NIH HHS/United States
- N01 WH42109/WH/WHI NIH HHS/United States
- N01 WH42122/WH/WHI NIH HHS/United States
- N01 WH32100/WH/WHI NIH HHS/United States
- N01 WH24152/WH/WHI NIH HHS/United States
- N01 WH32122/WH/WHI NIH HHS/United States
- N01 WH42118/WH/WHI NIH HHS/United States
- N01 WH42126/WH/WHI NIH HHS/United States
- N01 WH42123/WH/WHI NIH HHS/United States
- N01 WH32111/WH/WHI NIH HHS/United States
- N01 WH42116/WH/WHI NIH HHS/United States
- N01 WH42117/WH/WHI NIH HHS/United States
- N01 WH32105/WH/WHI NIH HHS/United States
- N01 WH42113/WH/WHI NIH HHS/United States
- N01 WH42107/WH/WHI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
