

Low diagnostic yield of elective coronary angiography
- PMID: 20220183
- PMCID: PMC3920593
- DOI: 10.1056/NEJMoa0907272
Low diagnostic yield of elective coronary angiography
Erratum in
- N Engl J Med. 2010 Jul 29;363(5):498
Abstract
Background: Guidelines for triaging patients for cardiac catheterization recommend a risk assessment and noninvasive testing. We determined patterns of noninvasive testing and the diagnostic yield of catheterization among patients with suspected coronary artery disease in a contemporary national sample.
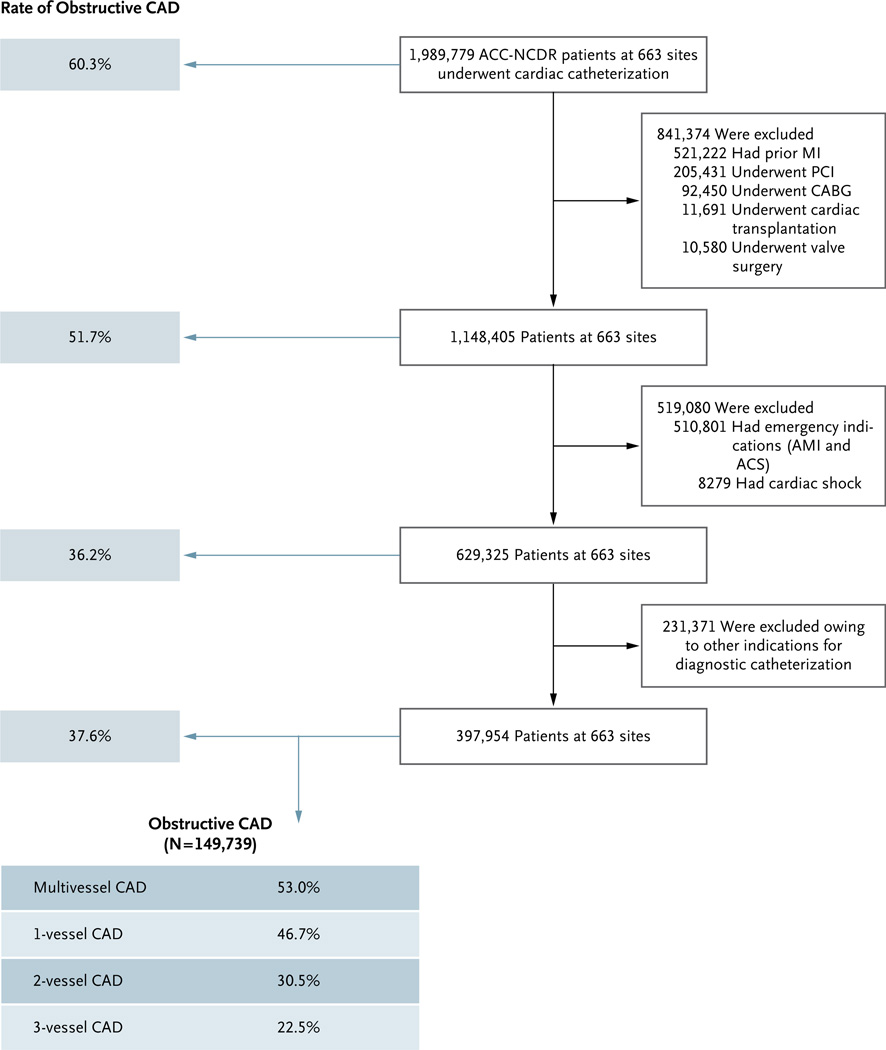
Methods: From January 2004 through April 2008, at 663 hospitals in the American College of Cardiology National Cardiovascular Data Registry, we identified patients without known coronary artery disease who were undergoing elective catheterization. The patients' demographic characteristics, risk factors, and symptoms and the results of noninvasive testing were correlated with the presence of obstructive coronary artery disease, which was defined as stenosis of 50% or more of the diameter of the left main coronary artery or stenosis of 70% or more of the diameter of a major epicardial vessel.
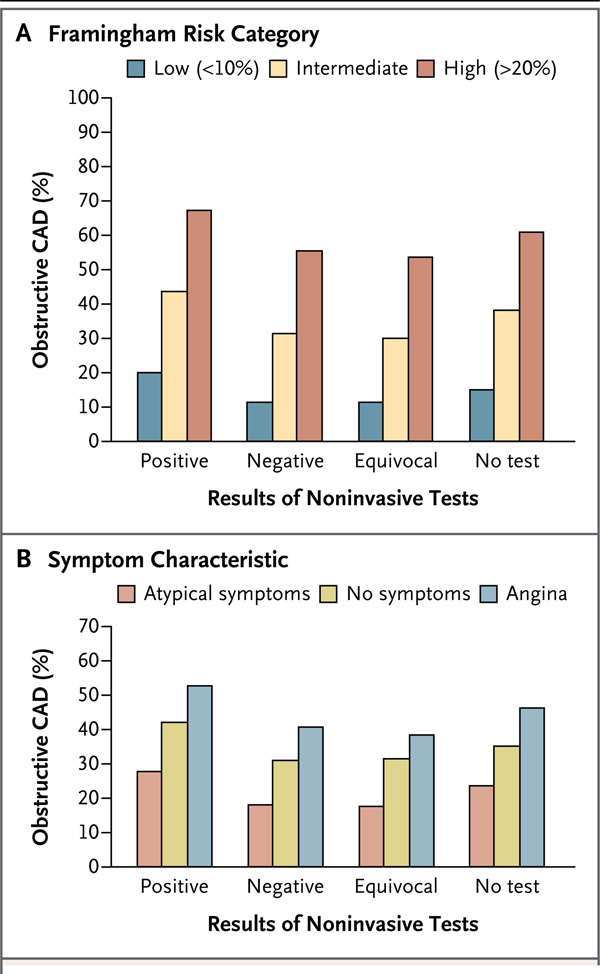
Results: A total of 398,978 patients were included in the study. The median age was 61 years; 52.7% of the patients were men, 26.0% had diabetes, and 69.6% had hypertension. Noninvasive testing was performed in 83.9% of the patients. At catheterization, 149,739 patients (37.6%) had obstructive coronary artery disease. No coronary artery disease (defined as <20% stenosis in all vessels) was reported in 39.2% of the patients. Independent predictors of obstructive coronary artery disease included male sex (odds ratio, 2.70; 95% confidence interval [CI], 2.64 to 2.76), older age (odds ratio per 5-year increment, 1.29; 95% CI, 1.28 to 1.30), presence of insulin-dependent diabetes (odds ratio, 2.14; 95% CI, 2.07 to 2.21), and presence of dyslipidemia (odds ratio, 1.62; 95% CI, 1.57 to 1.67). Patients with a positive result on a noninvasive test were moderately more likely to have obstructive coronary artery disease than those who did not undergo any testing (41.0% vs. 35.0%; P<0.001; adjusted odds ratio, 1.28; 95% CI, 1.19 to 1.37).
Conclusions: In this study, slightly more than one third of patients without known disease who underwent elective cardiac catheterization had obstructive coronary artery disease. Better strategies for risk stratification are needed to inform decisions and to increase the diagnostic yield of cardiac catheterization in routine clinical practice.
2010 Massachusetts Medical Society
Conflict of interest statement
No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
Medical imaging in the 21st century--getting the best bang for the rad.N Engl J Med. 2010 Mar 11;362(10):943-5. doi: 10.1056/NEJMe1000802. N Engl J Med. 2010. PMID: 20220190 No abstract available.
-
Low diagnostic yield of elective coronary angiography.N Engl J Med. 2010 Jul 1;363(1):92-3; author reply 94-5. doi: 10.1056/NEJMc1004220. N Engl J Med. 2010. PMID: 20592303 No abstract available.
-
Low diagnostic yield of elective coronary angiography.N Engl J Med. 2010 Jul 1;363(1):93; author reply 94-5. N Engl J Med. 2010. PMID: 20597149 No abstract available.
-
Low diagnostic yield of elective coronary angiography.N Engl J Med. 2010 Jul 1;363(1):93-4; author reply 94-5. N Engl J Med. 2010. PMID: 20597150 No abstract available.
-
Low diagnostic yield of elective coronary angiography.N Engl J Med. 2010 Jul 1;363(1):94; author reply 94-5. N Engl J Med. 2010. PMID: 20597151 No abstract available.
-
Is elective coronary angiography overused in patients with suspected coronary artery disease?Future Cardiol. 2010 Jul;6(4):455-7. doi: 10.2217/fca.10.26. Future Cardiol. 2010. PMID: 20608817
References
-
- Cheitlin MD, Armstrong WF, Aurigemma GP, et al. ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASE Committee to Update the 1997 Guidelines for the Clinical Application of Echocardiography) J Am Soc Echocardiogr. 2003;16:1091–1110. - PubMed
-
- Klocke FJ, Baird MG, Lorell BH, et al. ACC/AHA/ASNC guidelines for the clinical use of cardiac radionuclide imaging — executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/ASNC Committee to Revise the 1995 Guidelines for the Clinical Use of Cardiac Radionuclide Imaging) J Am Coll Cardiol. 2003;42:1318–1333. - PubMed
-
- Fraker TD, Jr, Fihn SD. 2007 Chronic angina focused update of the ACC/AHA 2002 guidelines for the management of patients with chronic stable angina: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Writing Group to develop the focused update of the 2002 guidelines for the management of patients with chronic stable angina. J Am Coll Cardiol. 2007;50:2264–2274. - PubMed
-
- Weintraub WS, McKay CR, Riner RN, et al. The American College of Cardiology National Database: progress and challenges. J Am Coll Cardiol. 1997;29:459–465. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous