

Clinical application of tumor volume in advanced nasopharyngeal carcinoma to predict outcome
- PMID: 20222940
- PMCID: PMC2842277
- DOI: 10.1186/1748-717X-5-20
Clinical application of tumor volume in advanced nasopharyngeal carcinoma to predict outcome
Abstract
Background: Current staging systems have limited ability to adjust optimal therapy in advanced nasopharyngeal carcinoma (NPC). This study aimed to delineate the correlation between tumor volume, treatment outcome and chemotherapy cycles in advanced NPC.
Methods: A retrospective review of 110 patients with stage III-IV NPC was performed. All patients were treated first with neoadjuvant chemotherapy, then concurrent chemoradiation, and followed by adjuvant chemotherapy as being the definitive therapy. Gross tumor volume of primary tumor plus retropharyngeal nodes (GTVprn) was calculated to be an index of treatment outcome.
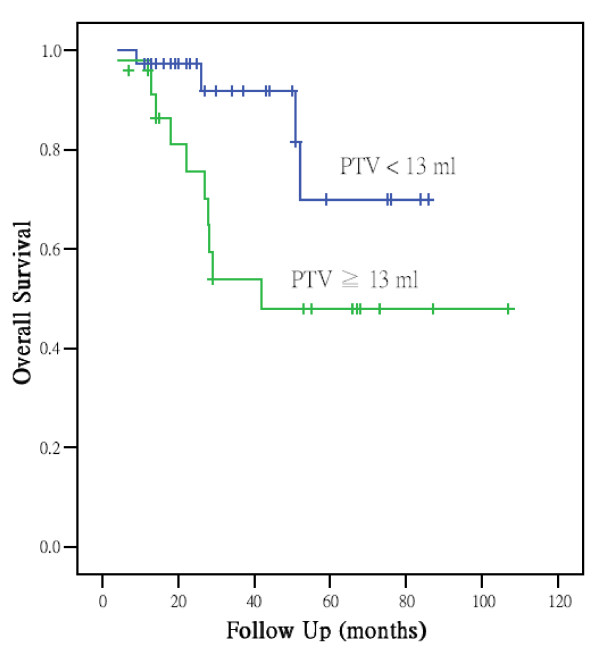
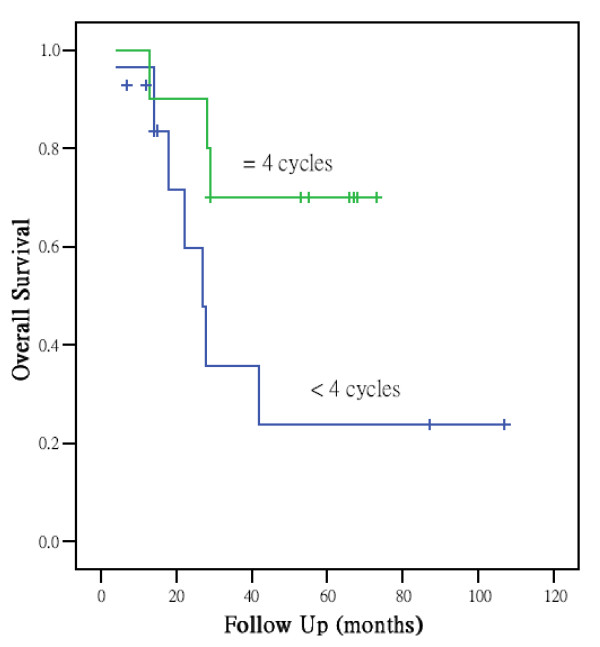
Results: GTVprn had a close relationship with survival and recurrence in advanced NPC. Large GTVprn (> or =13 ml) was associated with a significantly poorer local control, lower distant metastasis-free rate, and poorer survival. In patients with GTVprn > or =13 ml, overall survival was better after > or =4 cycles of chemotherapy than after less than 4 cycles.
Conclusions: The incorporation of GTVprn can provide more information to adjust treatment strategy.
Figures
Similar articles
-
Concurrent chemoradiotherapy with adjuvant chemotherapy for high-risk nasopharyngeal carcinoma.Auris Nasus Larynx. 2009 Dec;36(6):688-94. doi: 10.1016/j.anl.2009.03.009. Epub 2009 May 1. Auris Nasus Larynx. 2009. PMID: 19410399
-
A comparative study of locoregionally advanced nasopharyngeal carcinoma treated with intensity modulated irradiation and platinum-based chemotherapy.Cancer Radiother. 2013 Jul-Aug;17(4):297-303. doi: 10.1016/j.canrad.2013.03.006. Epub 2013 Jul 9. Cancer Radiother. 2013. PMID: 23849438
-
Intensity-modulated radiation therapy without concurrent chemotherapy for stage IIb nasopharyngeal cancer.Am J Clin Oncol. 2010 Jun;33(3):294-9. doi: 10.1097/COC.0b013e3181d2edab. Am J Clin Oncol. 2010. PMID: 20395788
-
Concurrent chemoradiotherapy in locally advanced nasopharyngeal carcinoma: a treatment paradigm also applicable to patients in Southeast Asia.Cancer Treat Rev. 2009 Jun;35(4):345-53. doi: 10.1016/j.ctrv.2009.01.002. Epub 2009 Feb 10. Cancer Treat Rev. 2009. PMID: 19211192 Review.
-
Treatment for metastatic nasopharyngeal carcinoma.Eur Ann Otorhinolaryngol Head Neck Dis. 2011 Apr;128(2):79-85. doi: 10.1016/j.anorl.2010.10.003. Epub 2010 Dec 21. Eur Ann Otorhinolaryngol Head Neck Dis. 2011. PMID: 21177151 Review.
Cited by
-
Is maximum primary tumor diameter still a prognostic factor in patients with nasopharyngeal carcinoma treated using intensity-modulated radiotherapy?BMC Cancer. 2015 Apr 18;15:305. doi: 10.1186/s12885-015-1288-8. BMC Cancer. 2015. PMID: 25903652 Free PMC article.
-
[Down-regulation of miR-205-5p enhances pro-apoptotic effect of 3-bromopyruvate on human nasopharyngeal carcinoma CNE2Z cells].Nan Fang Yi Ke Da Xue Xue Bao. 2019 Oct 30;39(10):1166-1172. doi: 10.12122/j.issn.1673-4254.2019.10.06. Nan Fang Yi Ke Da Xue Xue Bao. 2019. PMID: 31801705 Free PMC article. Chinese.
-
Validation of bidimensional measurement in nasopharyngeal carcinoma.Radiat Oncol. 2010 Aug 16;5:72. doi: 10.1186/1748-717X-5-72. Radiat Oncol. 2010. PMID: 20712871 Free PMC article.
-
Pretreatment Dynamic Contrast-Enhanced MRI Improves Prediction of Early Distant Metastases in Patients With Nasopharyngeal Carcinoma.Medicine (Baltimore). 2016 Feb;95(6):e2567. doi: 10.1097/MD.0000000000002567. Medicine (Baltimore). 2016. PMID: 26871776 Free PMC article.
-
Baseline tumour measurements predict survival in advanced non-small cell lung cancer.Br J Cancer. 2013 Sep 17;109(6):1476-81. doi: 10.1038/bjc.2013.472. Epub 2013 Aug 13. Br J Cancer. 2013. PMID: 23942074 Free PMC article. Clinical Trial.
References
-
- Greene FL, Page DL, Fleming ID, Fritz A, Balch CM, Haller DG, Morrow M. AJCC Cancer Staging Manual. 6. New York: Springer-Verlag; 2002. pp. 47–52.
MeSH terms
LinkOut - more resources
Full Text Sources
