

Pre-hospital ECG for acute coronary syndrome in urban India: a cost-effectiveness analysis
- PMID: 20222987
- PMCID: PMC2848184
- DOI: 10.1186/1471-2261-10-13
Pre-hospital ECG for acute coronary syndrome in urban India: a cost-effectiveness analysis
Abstract
Background: Patients with acute coronary syndrome (ACS) in India have increased pre-hospital delay and low rates of thrombolytic reperfusion. Use of ECG could reduce pre-hospital delay among patients who first present to a general practitioner (GP). We assessed whether performing ECG on patients with acute chest pain would improve long-term outcomes and be cost-effective.
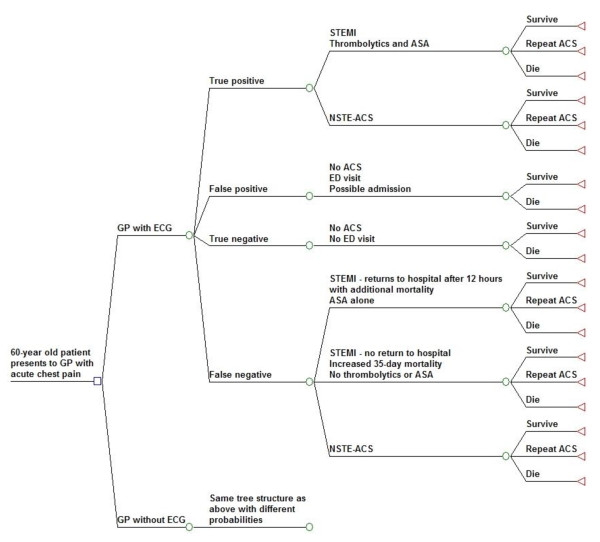
Methods: We created a Markov model of urban Indian patients presenting to a GP with acute chest pain to compare a GP's performing an ECG versus not performing one. Variables describing the accuracy of a GP's referral decision in chest pain and ACS, ACS treatment patterns, the effectiveness of thrombolytic reperfusion, and costs were derived from Indian data where available and other developed world studies. The model was used to estimate the incremental cost-effectiveness ratio (ICER) of the intervention in 2007 US dollars per quality adjusted life years (QALY) gained.
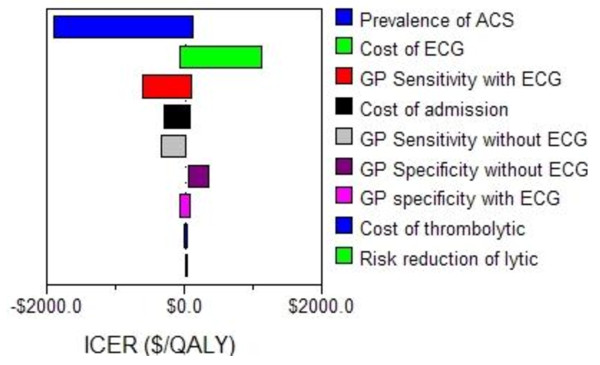
Results: Under baseline assumptions, the ECG strategy cost an additional $12.65 per QALY gained compared to no ECG. Sensitivity analyses around the cost of the ECG, cost of thrombolytic, and referral accuracy of the GP yielded ICERs for the ECG strategy ranging between cost-saving and $1124/QALY. All results indicated the intervention is cost-effective under current World Health Organization recommendations.
Conclusions: While direct presentation to the hospital with acute chest pain is preferable, in urban Indian patients presenting first to a GP, an ECG performed by the GP is a cost-effective strategy to reduce disability and mortality. This strategy should be clinically studied and considered until improved emergency transport services are available.
Figures
References
-
- Ezzati M, Lopez AD, Rodgers A, Murray CJL. Comparative quantification of health risks. Global and regional burden of disease attributable to major risk factors. Geneva: World Health Organization; 2004.
-
- Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, Hochman JS, Krumholz HM, Kushner FG, Lamas GA. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction) Circulation. 2004;110(9):e82–292. - PubMed
-
- API expert consensus document on management of ischemic heart disease. J Assoc Physicians India. 2006;54:469–480. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
