

An introduction to managing medullary thyroid cancer
- PMID: 20223015
- PMCID: PMC4177236
- DOI: 10.1186/1897-4287-4-3-115
An introduction to managing medullary thyroid cancer
Abstract
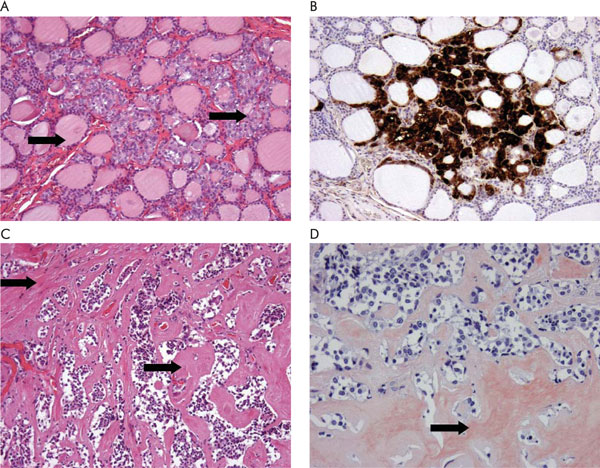
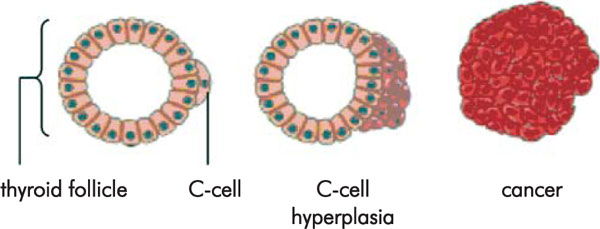
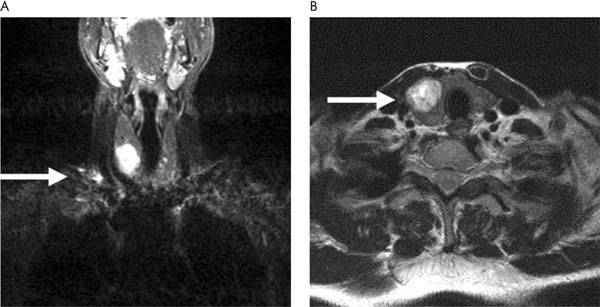
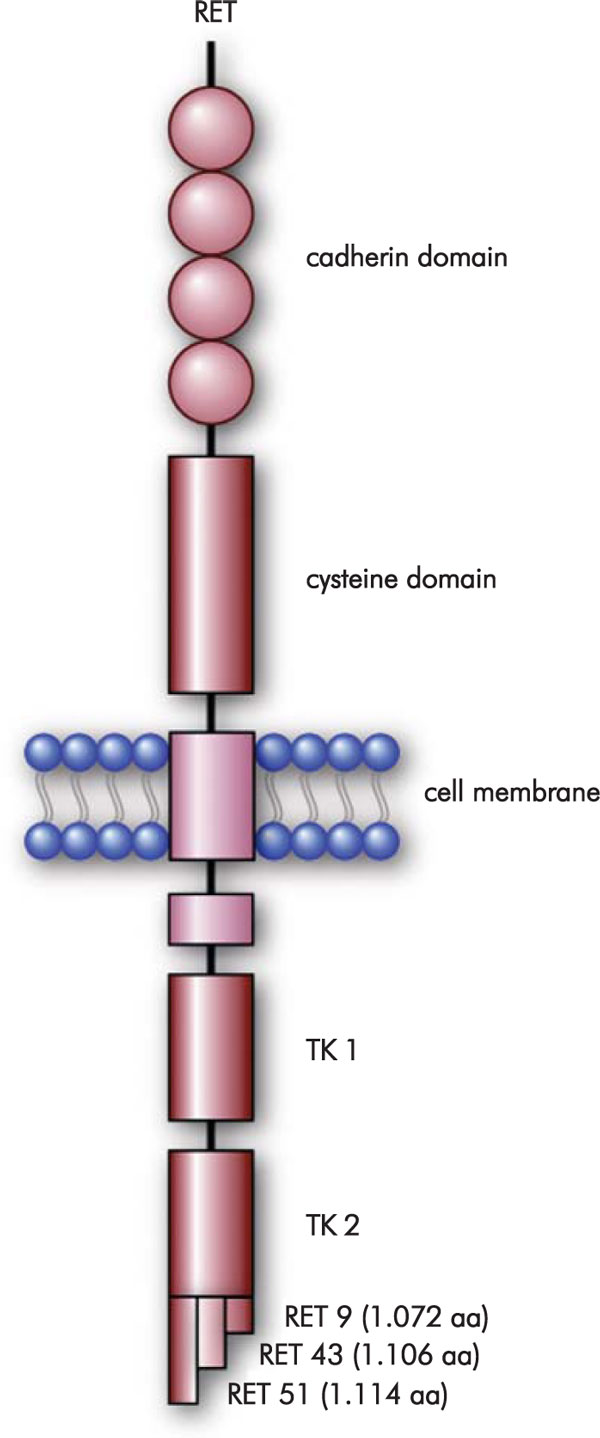
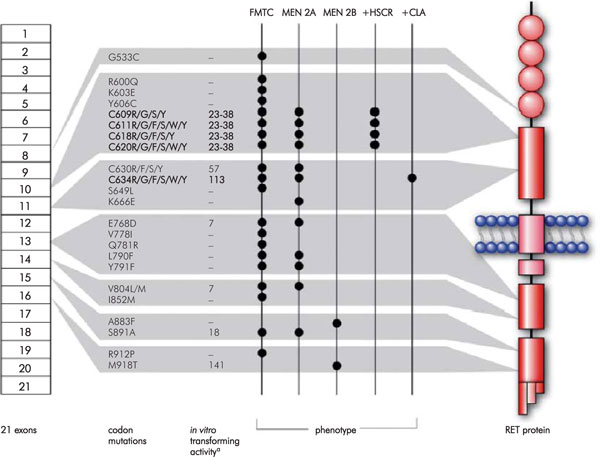
MTC is a rare neuroendocrine thyroid tumour accounting for 3% to 10% of all thyroid malignancies. It can occur in a sporadic and a hereditary clinical setting. Hereditary MTC may either occur alone (familial MTC, FMTC) or as part of multiple endocrine neoplasia (MEN) type 2A, or MEN 2B. These disorders are due to germline mutations in the RET (REarranged during Transfection) gene. In carriers of MEN 2B-associated RET mutations, prophylactic thyroidectomy is indicated before the first year of life. In the case of MEN 2A-associated germline RET mutations with a high-risk profile, total thyroidectomy is warranted before the age of 2 years and certainly before the age of 4 years. At that age the risk of invasive MTC and metastases is acceptably low. Depending on the type of RET mutation, thyroidectomy can take place at an older age in patients with a lower risk profile. In case of elevated basal or stimulated serum calcitonin, preventive surgery including total thyroidectomy and central compartment dissection should be performed regardless of age. When MTC presents as a palpable tumour, total thyroidectomy should be combined with extensive lymph node dissection of levels II-V on both sides and level VI to prevent locoregional recurrences.
Figures
Similar articles
-
Clinical utility of genetic diagnosis for sporadic and hereditary medullary thyroid carcinoma.Ann Endocrinol (Paris). 2019 Jun;80(3):187-190. doi: 10.1016/j.ando.2019.04.014. Epub 2019 Apr 11. Ann Endocrinol (Paris). 2019. PMID: 31053251
-
A Nationwide Study of Multiple Endocrine Neoplasia Type 2A in Norway: Predictive and Prognostic Factors for the Clinical Course of Medullary Thyroid Carcinoma.Thyroid. 2016 Sep;26(9):1225-38. doi: 10.1089/thy.2015.0673. Epub 2016 Aug 11. Thyroid. 2016. PMID: 27400880
-
Medullary thyroid carcinoma in children with multiple endocrine neoplasia types 2A and 2B.J Pediatr Surg. 1996 Jan;31(1):177-81; discussion 181-2. doi: 10.1016/s0022-3468(96)90343-7. J Pediatr Surg. 1996. PMID: 8632274
-
[Prophylactic thyroidectomy in children who are carriers of a multiple endocrine neoplasia type 2 mutation: description of 20 cases and recommendations based on the literature].Ned Tijdschr Geneeskd. 2006 Feb 11;150(6):311-8. Ned Tijdschr Geneeskd. 2006. PMID: 16503023 Review. Dutch.
-
Medullary carcinoma of the thyroid gland and the MEN 2 syndromes.Semin Pediatr Surg. 1997 Aug;6(3):134-40. Semin Pediatr Surg. 1997. PMID: 9263335 Review.
References
LinkOut - more resources
Full Text Sources