

Evaluation of the introduction of a standardised protocol for the staging and follow-up of colorectal cancer on resection rates for liver metastases
- PMID: 20223052
- PMCID: PMC3080067
- DOI: 10.1308/003588410X12628812458419
Evaluation of the introduction of a standardised protocol for the staging and follow-up of colorectal cancer on resection rates for liver metastases
Abstract
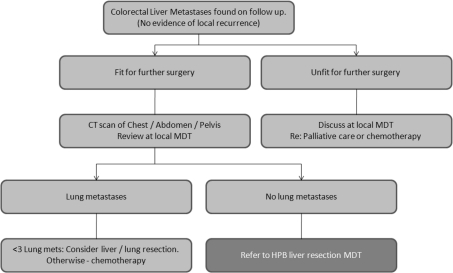
Introduction: In 2004, an audit in our unit demonstrated wide variation in liver resection rates for colorectal cancer (CRC) metastases within the cancer network. Subsequently, a network-wide CT-based follow-up and referral policy was introduced for all patients. A second audit was performed to assess the impact of the guidelines on liver resection rates.
Subjects and methods: Analysis of prospective liver resection database between 1997 and 2004 and after the introduction of standardised guidelines between January 2005 and April 2008.
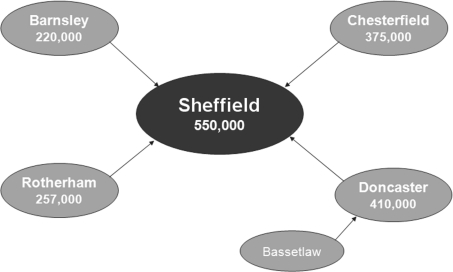
Results: A total of 362 patients underwent liver resection for CRC metastases between 1997 and 2008, 237 prior to the introduction of the referral guidelines and 125 after. Liver resection rates according to referring hospital varied from 0.92 to 2.32 per 100,000 population before guidelines were introduced. After 2005, resection rates from the four district hospitals standardised (1.68-1.84 per 100,000 population), but the central unit rate (Sheffield) remained significantly higher (2.67 per 100,000 population). No significant difference in 1-year disease-free survival between patients from Sheffield and the out-lying hospitals was found (P = 0.553).
Conclusions: Introduction of a referral protocol standardised resection rates from the four district hospitals, but these remain lower compared to the specialist centre. The wide-spread adoption of a policy to discuss all patients with liver metastases at an advanced disease multidisciplinary team meeting, in the presence of hepatobiliary specialists, may further increase resection rates across the UK.
Figures
References
-
- Westlake S, Cooper N. Cancer incidence and mortality: trends in the United Kingdom and constituent countries, 1993 to 2004. Health Stat Q. 2008;38:33–46. - PubMed
-
- Galandiuk S, Wieand HS, Moertel CG, Cha SS, Fitzgibbons Jr RJ, et al. Patterns of recurrence after curative resection of carcinoma of the colon and rectum. Surg Gynecol Obstet. 1992;174:27–32. - PubMed
-
- Fusai G, Davidson BR. Management of colorectal liver metastases. Colorectal Dis. 2003;5:2–23. - PubMed
-
- Wicherts DA, de Haas RJ, Adam R. Bringing unresectable liver disease to resection with curative intent. Eur J Surg Oncol. 2007;33(Suppl 2):S42–51. - PubMed
-
- Lord J, Shaw L, Dobbs F, Acharya U. A time for change and a time for equality – infertility services and the NHS. Hum Fertil (Camb) 2001;4:256–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous