

Mechanical strength of the side-to-side versus Pulvertaft weave tendon repair
- PMID: 20223604
- PMCID: PMC2852184
- DOI: 10.1016/j.jhsa.2010.01.009
Mechanical strength of the side-to-side versus Pulvertaft weave tendon repair
Abstract
Purpose: The side-to-side (SS) tendon suture technique was designed to function as a repair that permits immediate postoperative activation and mobilization of a transferred muscle. This study was designed to test the strength and stiffness of the SS technique against a variation of the Pulvertaft (PT) repair technique.
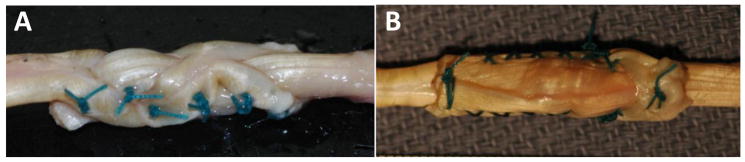
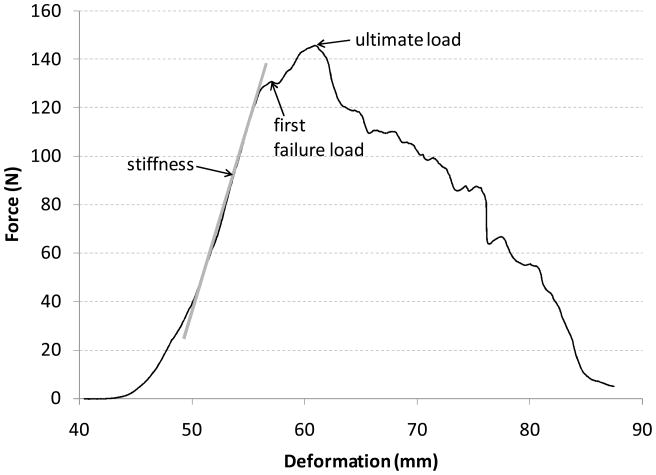
Methods: Flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons were harvested from 4 fresh cadavers and used as a model system. Seven SS and 6 PT repairs were performed, using the FDS as the donor and the FDP as the recipient tendon. For SS repairs, the FDS was woven through one incision in the FDP and was joined with 4 cross-stitch running sutures down both sides and one double-loop suture at each tendon free end. For PT repairs, the FDS was woven through 3 incisions in the FDP and joined with a double-loop suture at both ends of the overlap and 4 evenly spaced mattress sutures between the ends. Tendon repairs were placed in a tensile testing machine, preconditioned, and tested to failure.
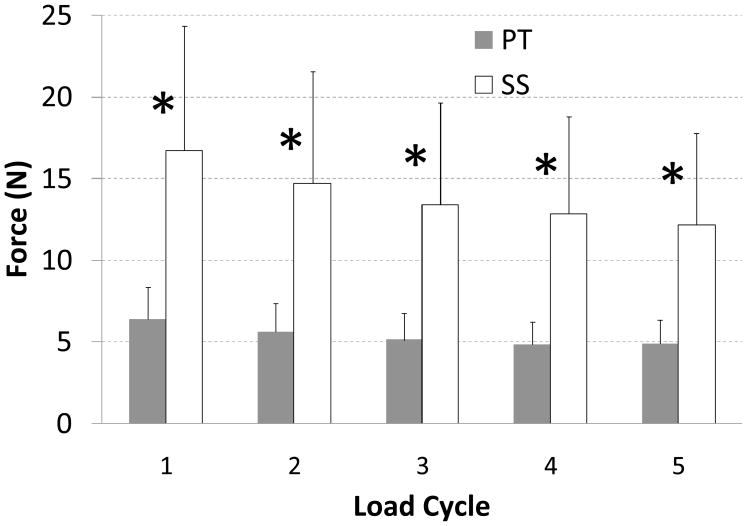
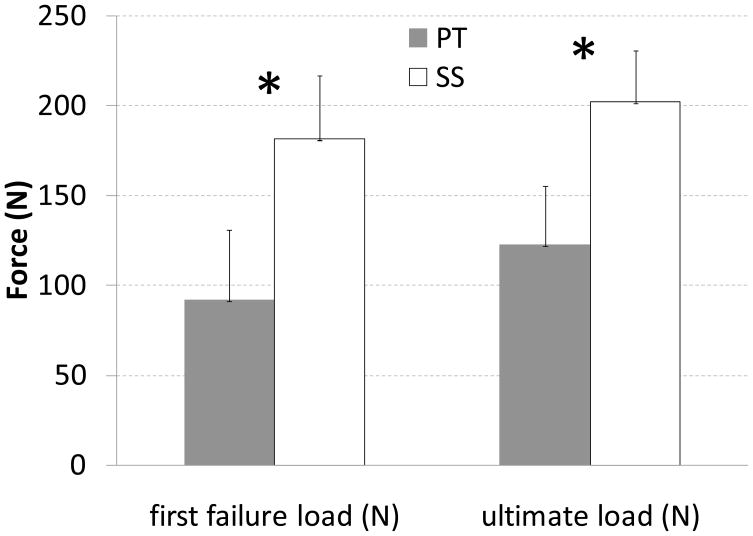
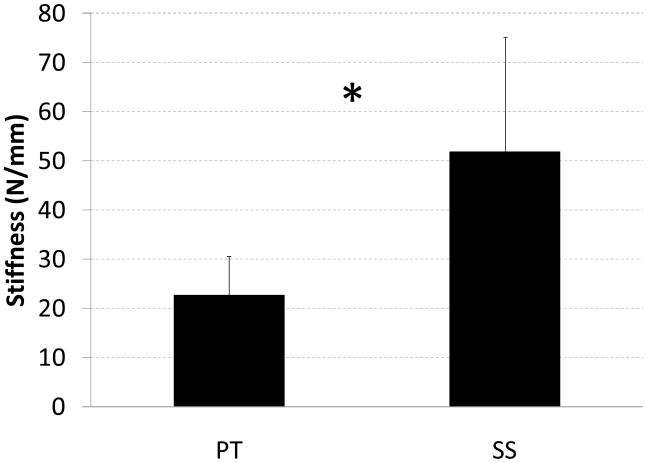
Results: There were no statistically significant differences in cross-sectional area (p = .99) or initial length (p = .93) between SS and PT repairs. Therefore, all comparisons between methods were made using measures of loads and deformations, rather than stresses and strains. All failures occurred in the repair region, rather than at the clamps. However, failure mechanisms were different between the 2 techniques-PT repairs failed by the suture knots either slipping or pulling through the tendon material, followed by the FDS tendon pulling through the FDP tendon; SS repairs failed by shearing of fibers within the FDS. Load at first failure, ultimate load, and repair stiffness were all significantly different between SS and PT techniques; in all cases, the mean value for SS was higher than for PT.
Conclusions: The SS repair using a cross-stitch suture technique was significantly stronger and stiffer than the PT repair using a mattress suture technique. This suggests that using SS repairs could enable patients to load the repair soon after surgery. Ultimately, this should reduce the risk of developing adhesions and result in improved functional outcome and fewer complications in the acute postoperative period. Future work will address the specific mechanisms (eg, suture-throw technique and tendon-weave technique) that underlie the improved strength and stiffness of the SS repair.
Figures
References
-
- Silfverskiöld KL, May EJ. Early active mobilization after tendon transfers using mesh reinforced suture techniques. J Hand Surg. 1995;20B:291–300. - PubMed
-
- Rath S. Immediate postoperative active mobilization versus immobilization following tendon transfer for claw deformity correction in the hand. J Hand Surg. 2008;33A:232–240. - PubMed
-
- Doi K, Hattori Y, Yamazaki H, Wahegaonkar AL, Addosooki A, Watanabe M. Importance of early passive mobilization following double free gracilis muscle transfer. Plast Reconstr Surg. 2008;121:2037–2045. - PubMed
-
- Gelberman RH, Woo SL, Lothringer K, Akeson WH, Amiel D. Effects of early intermittent passive mobilization on healing canine flexor tendons. J Hand Surg. 1982;7A:170–175. - PubMed
-
- Gelberman RH, Amiel D, Gonsalves M, Woo S, Akeson WH. The influence of protected passive mobilization on the healing of flexor tendons: a biochemical and microangiographic study. Hand. 1981;13:120–128. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
