

Supine cycling plus volume loading prevent cardiovascular deconditioning during bed rest
- PMID: 20223994
- PMCID: PMC3774511
- DOI: 10.1152/japplphysiol.01408.2009
Supine cycling plus volume loading prevent cardiovascular deconditioning during bed rest
Abstract
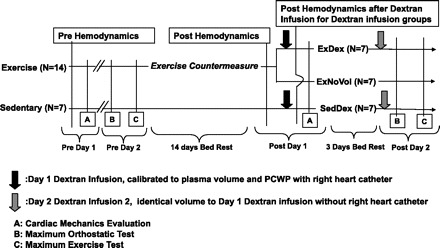
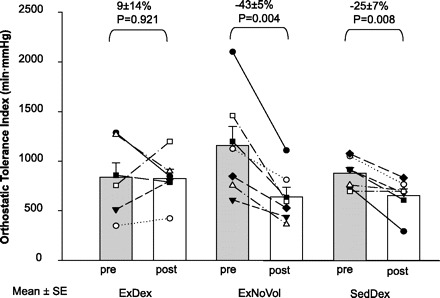
There are two possible mechanisms contributing to the excessive fall of stroke volume (and its contribution to orthostatic intolerance) in the upright position after bed rest or spaceflight: reduced cardiac filling due to hypovolemia and/or a less distensible heart due to cardiac atrophy. We hypothesized that preservation of cardiac mechanical function by exercise training, plus normalization of cardiac filling with volume infusion, would prevent orthostatic intolerance after bed rest. Eighteen men and three women were assigned to 1) exercise countermeasure (n=14) and 2) no exercise countermeasure (n=7) groups during bed rest. Bed rest occurred in the 6 degrees head-down tilt position for 18 days. The exercise regimen was prescribed to compensate for the estimated cardiac work reduction between bed rest and ambulatory periods. At the end of bed rest, the subjects were further divided into two additional groups for post-bed rest testing: 1) volume loading with intravenous dextran to normalize cardiac filling pressure and 2) no volume loading. Dextran infusion was given to half of the exercise group and all of the sedentary group after bed rest, leading ultimately to three groups: 1) exercise plus volume infusion; 2) exercise alone; and 3) volume infusion alone. Exercise training alone preserved left ventricular mass and distensibility as well as upright exercise capacity, but lower body negative pressure (LBNP) tolerance was still depressed. LBNP tolerance was maintained only when exercise training was accompanied by dextran infusion. Dextran infusion alone following bed rest without exercise maintained neither orthostatic tolerance nor upright exercise capacity. We conclude that daily supine cycle exercise sufficient to prevent cardiac atrophy can prevent orthostatic intolerance after bed rest only when combined with plasma volume restoration. This maintenance of orthostatic tolerance was achieved by neither exercise nor dextran infusion alone. Cardiac atrophy and hypovolemia are likely to contribute independently to orthostatic intolerance after bed rest.
Figures


References
-
- Arbab-Zadeh A, Dijk E, Prasad A, Fu Q, Torres P, Zhang R, Thomas JD, Palmer D, Levine BD. Effect of aging and physical activity on left ventricular compliance. Circulation 110: 1799–1805, 2004 - PubMed
-
- Blomqvist C, Stone H. Cardiovascular adjustments to gravitational stress. In: Handbook of Physiology. The Cardiovascular System. Bethesda, MD: Am Physiol Soc, 1983, sect. 2, vol. III, pt. 2, p. 1025–1063
-
- Buckey JC, Jr, Lane LD, Levine BD, Watenpaugh DE, Wright SJ, Moore WE, Gaffney FA, Blomqvist CG. Orthostatic intolerance after spaceflight. J Appl Physiol 81: 7–18, 1996 - PubMed
-
- Bungo MW, Charles JB, Johnson PC., Jr Cardiovascular deconditioning during space flight and the use of saline as a countermeasure to orthostatic intolerance. Aviat Space Environ Med 56: 985–990, 1985 - PubMed
-
- Connolly D, Kirklin J, Wood E. The relationship between pulmonary artery wedge pressure and left atrial pressure in man. Circ Res 2: 434–440, 1954 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources