

Beyond mortality: future clinical research in acute lung injury
- PMID: 20224063
- PMCID: PMC2874454
- DOI: 10.1164/rccm.201001-0024WS
Beyond mortality: future clinical research in acute lung injury
Abstract
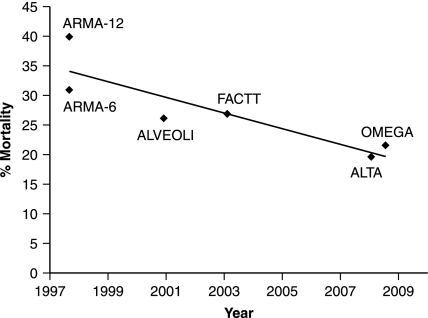
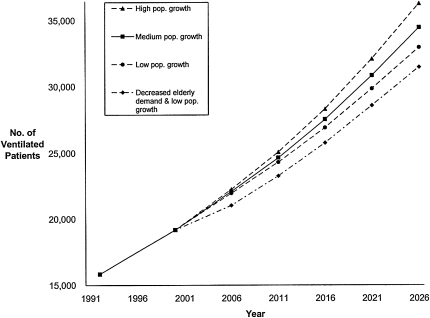
Mortality in National Heart, Lung and Blood Institute-sponsored clinical trials of treatments for acute lung injury (ALI) has decreased dramatically during the past two decades. As a consequence, design of such trials based on a mortality outcome requires ever-increasing numbers of patients. Recognizing that advances in clinical trial design might be applicable to these trials and might allow trials with fewer patients, the National Heart, Lung and Blood Institute convened a workshop of extramural experts from several disciplines. The workshop assessed the current state of clinical research addressing ALI, identified research needs, and recommended: (1) continued performance of trials evaluating treatments of patients with ALI; (2) development of strategies to perform ALI prevention trials; (3) observational studies of patients without ALI undergoing prolonged mechanical ventilation; and (4) development of a standardized format for reporting methods, endpoints, and results of ALI trials.
Figures
References
-
- Zambon M, Vincent JL. Mortality rates for patients with acute lung injury/ARDS have decreased over time. Chest 2008;133:1120–1127. - PubMed
-
- Phua J, Badia JR, Adhikari NK, Friedrich JO, Fowler RA, Singh JM, Scales DC, Stather DR, Li A, Jones A, et al. Has mortality from acute respiratory distress syndrome decreased over time?: a systematic review. Am J Respir Crit Care Med 2009;179:220–227. - PubMed
-
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000;342:1301–1308. - PubMed
-
- Brower RG, Lanken PN, MacIntyre N, Matthay MA, Morris A, Ancukiewicz M, Schoenfeld D, Thompson BT. Higher versus lower positive end-expiratory pressures in patients with the acute respiratory distress syndrome. N Engl J Med 2004;351:327–336. - PubMed
-
- Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, deBoisblanc B, Connors AFJ, Hite RD, Harabin AL. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006;354:2564–2575. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
