

Predictors of timely antibiotic administration for patients hospitalized with community-acquired pneumonia from the cluster-randomized EDCAP trial
- PMID: 20224313
- PMCID: PMC2875077
- DOI: 10.1097/MAJ.0b013e3181d3cd63
Predictors of timely antibiotic administration for patients hospitalized with community-acquired pneumonia from the cluster-randomized EDCAP trial
Abstract
Introduction: To identify factors associated with timely initiation of antibiotic therapy for patients hospitalized with pneumonia.
Design: Secondary analysis of a cluster-randomized, controlled trial.
Setting: Thirty- two emergency departments (EDs) in Pennsylvania and Connecticut.
Subjects: Patients with a clinical and radiographic diagnosis of community-acquired pneumonia.
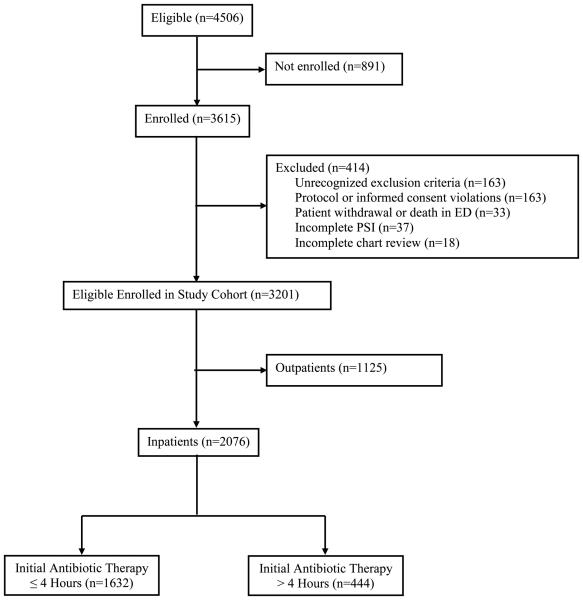
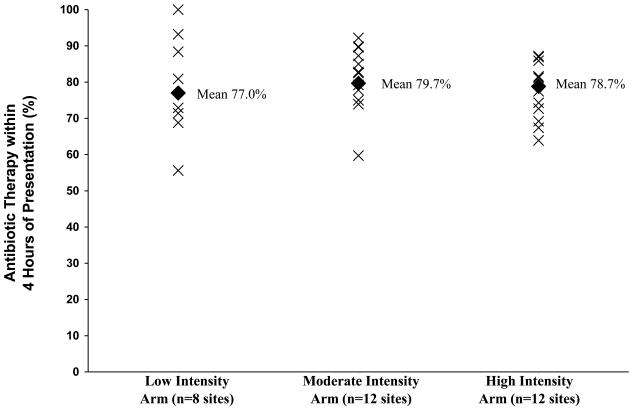
Interventions: From January to December 2001, EDs were randomly allocated to guideline implementation strategies of low (n = 8), moderate (n = 12), and high intensity (n = 12) to improve the initial site of treatment and the performance of evidence-based processes of care. Our primary outcome was antibiotic initiation within 4 hours of presentation, which at that time was the recommended process of care for inpatients.
Results: Of the 2076 inpatients enrolled, 1632 (78.6%) received antibiotic therapy within 4 hours of presentation. Antibiotic timeliness ranged from 55.6% to 100% (P < 0.001) by ED and from 77.0% to 79.7% (P = 0.2) across the 3 guideline implementation arms. In multivariable analysis, heart rate > or =125 per minute (OR = 1.6, 95% CI 1.1-2.3), respiratory rate > or =30 per minute (OR = 2.3, 95% CI 1.6-3.4), and aspiration pneumonia (OR = 3.7, 95% CI 1.1-12.7) were positively associated with timely initiation of antibiotic therapy, whereas a hematocrit <30% (OR = 0.6, 95% CI 0.4-1.0) was negatively associated with this outcome.
Conclusions: Timely initiation of antibiotic therapy is associated primarily with patient-related factors that reflect severity of illness at presentation. Although this study demonstrates an opportunity to improve performance on this quality measure in nearly one quarter of inpatients with pneumonia, we failed to identify any modifiable patient, provider, or hospital level factors to target in such quality improvement efforts.
Figures
References
-
- ERS Task Force Report Guidelines for management of adult community-acquired lower respiratory tract infections. European Respiratory Society. Eur Respir J. 1998;11:986–91. - PubMed
-
- Battleman DS, Callahan M, Thaler HT. Rapid antibiotic delivery and appropriate antibiotic selection reduce length of hospital stay of patients with community-acquired pneumonia: link between quality of care and resource utilization. Arch Intern Med. 2002;162:682–8. - PubMed
-
- Houck PM, Bratzler DW, Nsa W, Ma A, Bartlett JG. Timing of antibiotic administration and outcomes for Medicare patients hospitalized with community-acquired pneumonia. Arch Intern Med. 2004;164:637–44. - PubMed
-
- Meehan TP, Fine MJ, Krumholz HM, et al. Quality of care, process, and outcomes in elderly patients with pneumonia. JAMA. 1997;278:2080–4. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
