

Readmission after colectomy for cancer predicts one-year mortality
- PMID: 20224370
- PMCID: PMC2951007
- DOI: 10.1097/SLA.0b013e3181d3d27c
Readmission after colectomy for cancer predicts one-year mortality
Abstract
Objectives: Early hospital readmission is a common and costly problem in the Medicare population. In 2009, the Centers for Medicaid and Medicare Services began mandating hospital reporting of disease-specific readmission rates. We sought to determine the rate and predictors of readmission after colectomy for cancer, as well as the association between readmission and mortality.
Methods: Medicare beneficiaries who underwent colectomy for stage I to III colon adenocarcinoma from 1992 to 2002 were identified from the Surveillance, Epidemiology, and End Results-Medicare database. Multivariate logistic regression identified predictors of early readmission and 1-year mortality. Odds ratios were adjusted for multiple factors, including measures of comorbidity, socioeconomic status, and disease severity.
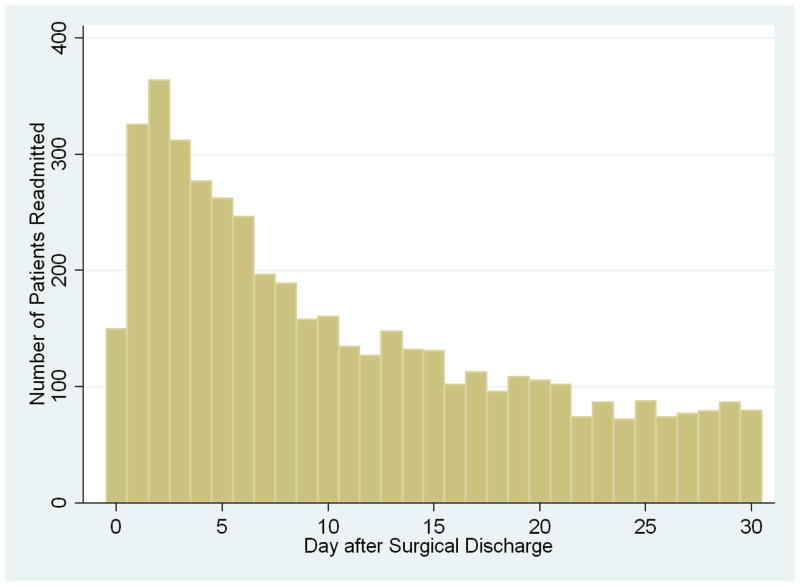
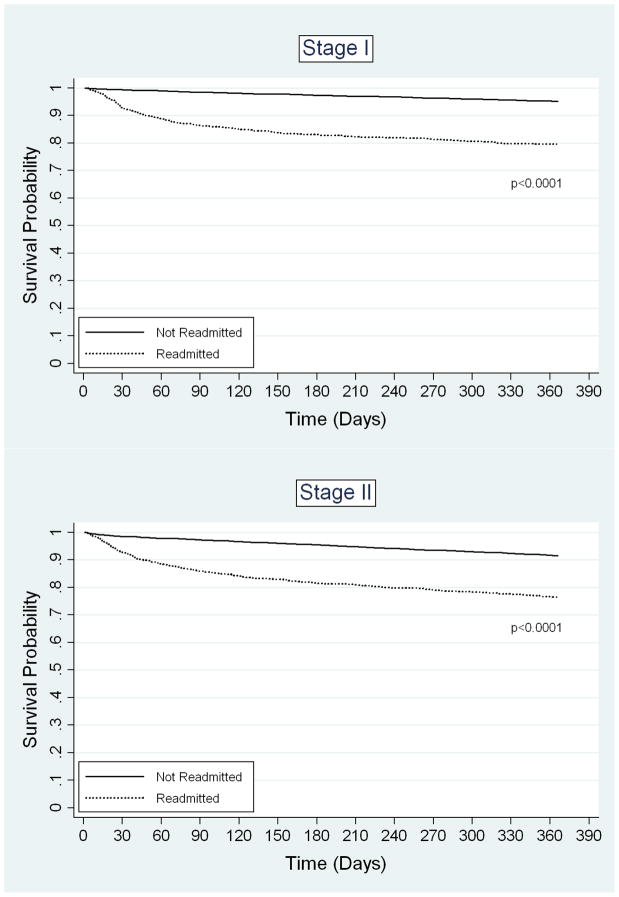
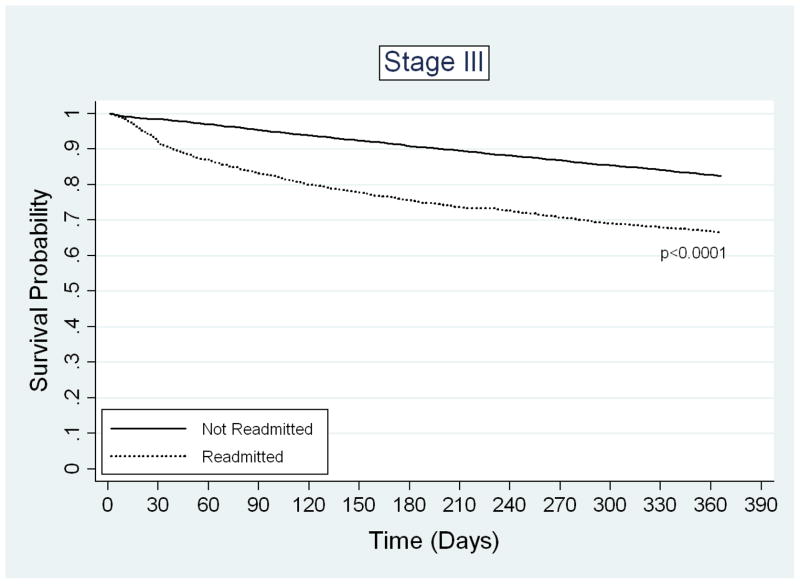
Results: Of 42,348 patients who were discharged, 4662 (11.0%) were readmitted within 30 days. The most common causes of rehospitalization were ileus/obstruction and infection. Significant predictors of readmission included male gender, comorbidity, emergent admission, prolonged hospital stay, blood transfusion, ostomy, and discharge to nursing home. Readmission was inversely associated with hospital procedure volume, but not surgeon volume. After adjusting for potential confounding variables, the predicted probability of 1-year mortality was 16% for readmitted patients, compared with 7% for those not readmitted. This difference in mortality was significant for all stages of cancer.
Conclusions: Early readmission after colectomy for cancer is common and due in part to modifiable factors. There is a remarkable association between readmission and 1-year mortality. Early readmission is therefore an important quality-of-care indicator for colon cancer surgery. These findings may facilitate the development of targeted interventions that will decrease readmissions and improve patient outcomes.
Figures
References
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. - PubMed
-
- Benbassat J, Taragin M. Hospital readmissions as a measure of quality of health care: advantages and limitations. Arch Intern Med. 2000;160:1074–1081. - PubMed
-
- Hennen J, Krumholz HM, Radford MJ, et al. Readmission rates, 30 days and 365 days postdischarge, among the 20 most frequent DRG groups, Medicare inpatients age 65 or older in Connecticut hospitals, fiscal years 1991, 1992, and 1993. Conn Med. 1995;59:263–270. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
