

Current guidelines for the management of asthma in young children
- PMID: 20224672
- PMCID: PMC2831604
- DOI: 10.4168/aair.2010.2.1.1
Current guidelines for the management of asthma in young children
Abstract
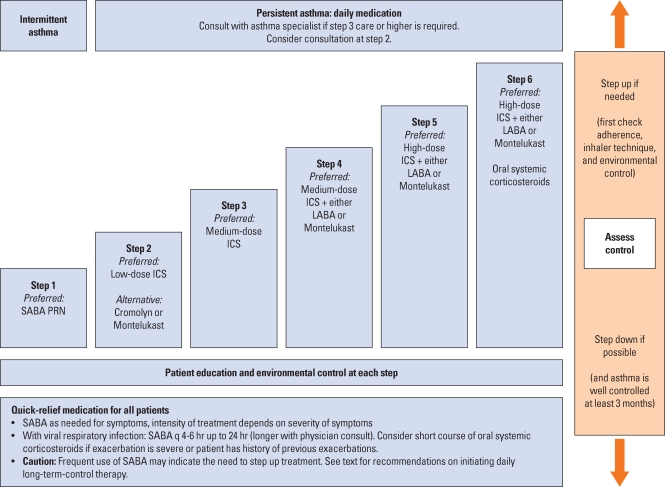
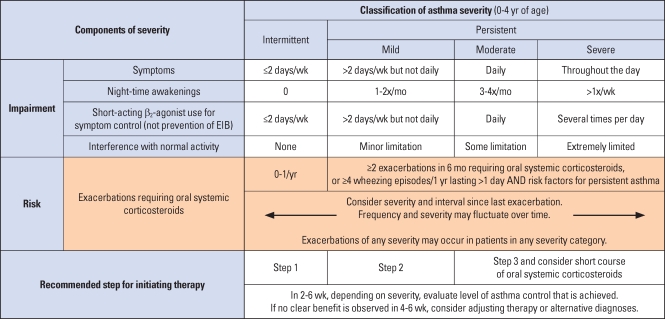
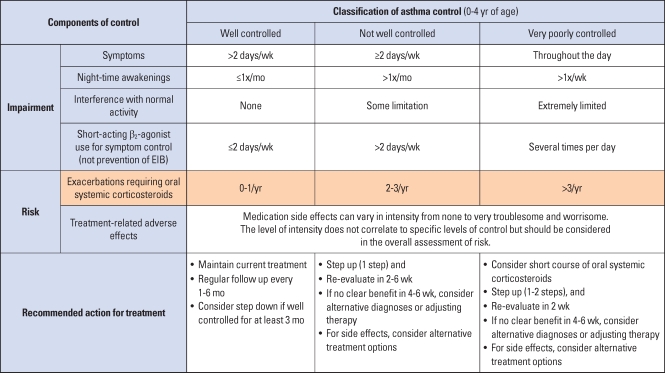
The diagnosis and management of asthma in young children is difficult, since there are many different wheezy phenotypes with varying underlying aetiologies and outcomes. This review discusses the different approaches to managing young children with wheezy illnesses presented in recently published global guidelines. Four major guidelines published since 2007 are considered. Helpful approaches are presented to assist the clinician to decide whether a clinical diagnosis of asthma can, or should be made in a young child with a recurrent wheezy illness and which treatments would be appropriate, dependent on risk factors, age of presentation, response to initial treatment and safety considerations. Each of the guidelines provide useful information for clinicians assessing young children with recurrent wheezy illnesses. There are differences in classification of the disease and treatment protocols. Although a firm diagnosis of asthma may only be made retrospectively in some cases and there are several effective guidelines to initiating treatment. Consistent review of the need for ongoing treatment with a particular pharmacological modality is essential, since many children with recurrent wheezing in infancy go into spontaneous remission. It is probable that newer biomarkers of airway inflammation will assist the clinician as to when to initiate and when to continue pharmacological treatment in the future.
Keywords: Asthma; guideline; preschool child.
Conflict of interest statement
There are no financial or other issues that might lead to conflict of interest.
Figures
References
-
- Asher MI, Montefort S, Bjorksten B, Lai CK, Strachan DP, Weiland SK, Williams H ISAAC Phase Three Study Group. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC Phases One and Three repeat multicountry cross-sectional surveys. Lancet. 2006;368:733–743. - PubMed
-
- EPR. Expert panel report: guidelines for the diagnosis and management of asthma (EPR 1991) Bethesda, MD: U.S. Department of Health and Human Services; National Institutes of Health; National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program; 1991. NIH Publication No. 91-3642.
-
- EPR-2. Expert panel report 2: guidelines for the diagnosis and management of asthma (EPR-2 1997) Bethesda, MD: U.S. Department of Health and Human Services; National Institutes of Health; National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program; 1997. NIH Publication No. 97-4051.
-
- EPR-Update 2002. Expert panel report: guidelines for the diagnosis and management of asthma. Update on selected topics 2002 (EPR-Update 2002) Bethesda, MD: U.S. Department of Health and Human Services; National Institutes of Health; National Heart, Lung, and Blood Institute; National Asthma Education and Prevention Program; 2003. Jun, NIH Publication No. 02 5074.
