

Treatment of unruptured intracranial aneurysms in South Korea in 2006 : a nationwide multicenter survey from the korean society of cerebrovascular surgery
- PMID: 20224709
- PMCID: PMC2836445
- DOI: 10.3340/jkns.2010.47.2.112
Treatment of unruptured intracranial aneurysms in South Korea in 2006 : a nationwide multicenter survey from the korean society of cerebrovascular surgery
Abstract
Objective: There have been no clinical studies regarding the epidemiology and treatment outcome for unruptured intracranial aneurysm (UIA) in South Korea yet. Thus, The Korean Society of Cerebrovascular Surgery (KSCVS) decided to evaluate the clinical and epidemiological characteristics, and outcome of the treatment of UIA in 2006, using the nationwide multicenter survey in South Korea.
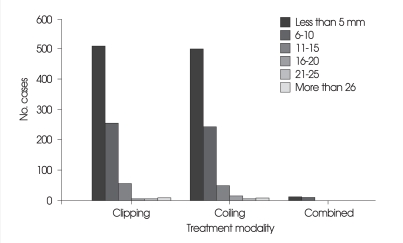
Methods: A total of 1,696 cases were enrolled retrospectively over one year at 48 hospitals. The following data were obtained from all patients : age, sex, presence of symptoms, location and size of the aneurysm, treatment modality, presence of risk factors for stroke, and the postoperative 30-day morbidity and mortality.
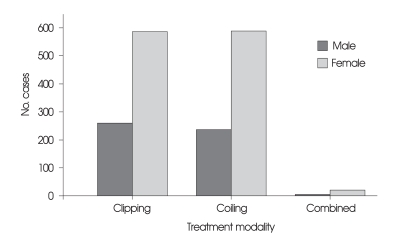
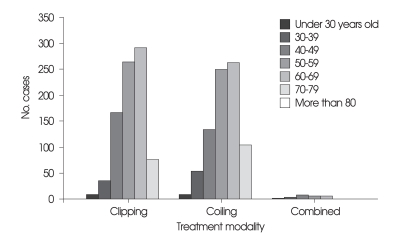
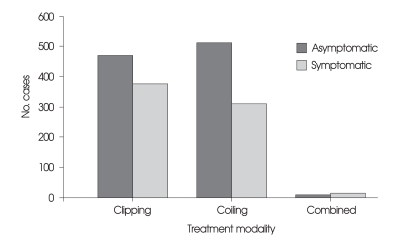
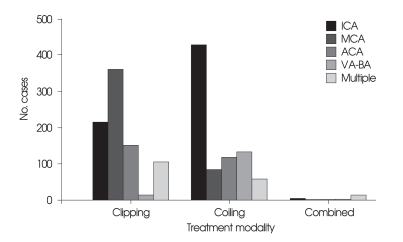
Results: The demographic data showed female predominance and peak age of seventh and sixth decades. Supraclinoid internal carotid artery was the most common site of aneurysms with a mean size of 5.6 mm. Eight-hundred-forty-six patients (49.9%) were treated with clipping, 824 (48.6%) with coiling, and 26 with combined method. The choice of the treatment modalities was related to hospital (p = 0.000), age (p = 0.000), presence of symptom (p = 0.003), and location of aneurysm (p = 0.000). The overall 30-day morbidity and mortality were 7.4% and 0.3%, respectively. The 30-day mortality was 0.4% for clipping and 0.2% for coiling, and morbidity was 8.4% for clipping and 6.3% for coiling. Age (p = 0.010), presence of symptoms (p = 0.034), size (p = 0.000) of aneurysm, and diabetes mellitus (p = 0.000) were significant prognostic factors, while treatment modality was not.
Conclusion: This first nation-wide multicenter survey on UIAs demonstrates the epidemiological and clinical characteristics, outcome and the prognostic factors of the treatment of UIAs in South Korea. The 30-day postoperative outcome for UIAs seems to be reasonable morbidity and mortality in South Korea.
Keywords: Aneurysm; Intracranial; Korea; Multicenter study; National survey; Treatment outcome; Unruptured.
Figures
Similar articles
-
Endovascular coil embolization of unruptured intracranial aneurysms: a Korean multicenter study.Acta Neurochir (Wien). 2014 May;156(5):847-54. doi: 10.1007/s00701-014-2033-9. Epub 2014 Mar 8. Acta Neurochir (Wien). 2014. PMID: 24610449
-
Unruptured aneurysms in the elderly: perioperative outcomes and cost analysis of endovascular coiling and surgical clipping.Neurosurg Focus. 2018 May;44(5):E4. doi: 10.3171/2018.1.FOCUS17714. Neurosurg Focus. 2018. PMID: 29712518
-
Validation of effectiveness of keyhole clipping in nonfrail elderly patients with unruptured intracranial aneurysms.J Neurosurg. 2017 Dec;127(6):1307-1314. doi: 10.3171/2016.9.JNS161634. Epub 2017 Jan 6. J Neurosurg. 2017. PMID: 28059648
-
Management of Small Incidental Intracranial Aneurysms.Neurosurg Clin N Am. 2017 Jul;28(3):389-396. doi: 10.1016/j.nec.2017.02.006. Neurosurg Clin N Am. 2017. PMID: 28600013 Review.
-
Risk factors for angiographic recurrence after treatment of unruptured intracranial aneurysms: Outcomes from a series of 178 unruptured aneurysms treated by regular coiling or surgery.J Neuroradiol. 2017 Sep;44(5):298-307. doi: 10.1016/j.neurad.2017.05.003. Epub 2017 Jun 8. J Neuroradiol. 2017. PMID: 28602498 Review.
Cited by
-
National Trends in the Treatment of Ruptured Cerebral Aneurysms in Korea Using an Age-adjusted Method.J Korean Med Sci. 2020 Oct 12;35(39):e323. doi: 10.3346/jkms.2020.35.e323. J Korean Med Sci. 2020. PMID: 33045768 Free PMC article.
-
Clinical practice guideline for the management of intracranial aneurysms.Neurointervention. 2014 Sep;9(2):63-71. doi: 10.5469/neuroint.2014.9.2.63. Epub 2014 Sep 3. Neurointervention. 2014. PMID: 25426300 Free PMC article. Review.
-
Natural History of Unruptured Intracranial Aneurysms : A Retrospective Single Center Analysis.J Korean Neurosurg Soc. 2016 Jan;59(1):11-6. doi: 10.3340/jkns.2016.59.1.11. Epub 2016 Jan 20. J Korean Neurosurg Soc. 2016. PMID: 26885281 Free PMC article.
-
Endovascular treatment for unruptured intracranial aneurysms in elderly patients: single-center report.AJNR Am J Neuroradiol. 2011 Jun-Jul;32(6):1087-90. doi: 10.3174/ajnr.A2458. Epub 2011 May 19. AJNR Am J Neuroradiol. 2011. PMID: 21596818 Free PMC article.
-
Benefits of surgical treatment for unruptured intracranial aneurysms in elderly patients.J Korean Neurosurg Soc. 2011 Jan;49(1):20-5. doi: 10.3340/jkns.2011.49.1.20. Epub 2011 Jan 31. J Korean Neurosurg Soc. 2011. PMID: 21494358 Free PMC article.
References
-
- Barker FG, 2nd, Amin-Hanjani S, Butler WE, Hoh BL, Rabinov JD, Pryor JC, et al. Age-dependent differences in short-term outcome after surgical or endovascular treatment of unruptured intracranial aneurysms in the United States, 1996-2000. Neurosurgery. 2004;54:18–28. discussion 28-30. - PubMed
-
- da Costa LB, Gunnarsson T, Wallace MC. Unruptured intracranial aneurysms : Natural history and management decisions. Neurosurg Focus. 2004;17:E6. - PubMed
-
- de la Monte SM, Moore GW, Monk MA, Hutchins GM. Risk factors for the development and rupture of intracranial berry aneurysms. Am J Med. 1985;78:957–964. - PubMed
-
- Feigin VL, Rinkel GJ, Lawes CM, Algra A, Bennett DA, van Gijn J, et al. Risk factors for subarachnoid hemorrhage : an updated systematic review of epidemiological studies. Stroke. 2005;36:2773–2780. - PubMed
LinkOut - more resources
Full Text Sources
