

Foveal-Sparing Scotomas in Advanced Dry Age-Related Macular Degeneration
Affiliations
- PMID: 20224750
- PMCID: PMC2836024
Item in Clipboard
Foveal-Sparing Scotomas in Advanced Dry Age-Related Macular Degeneration
J Vis Impair Blind.
.
Abstract
Foveal-sparing scotomas are common in advanced dry macular degeneration (geographic atrophy). Foveal preservation may be present for a number of years. Despite good visual acuity, these patients have reduced reading rates. Magnification may not be effective if the text becomes too large to "fit" within the central spared area.
Figures
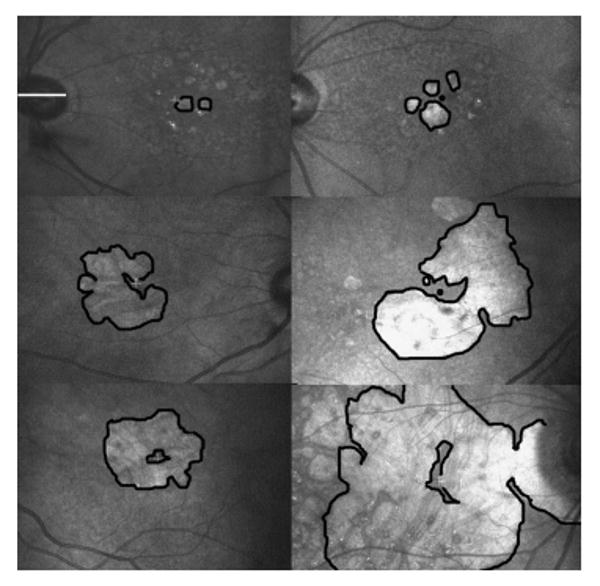
Scanning laser ophthalmoscope infrared images, showing configurations of GA from age-related macular degeneration with foveal sparing. The horizontal white line overlying the optic nerve in the upper left image is approximately 5 degrees in length, and all images are on the same scale. In each image, the borders of the larger areas of GA are outlined in black, so that the spared regions are outlined in black as well. The white fixation cross indicates the site of central fixation. In the images in which the fixation cross is not visible, a black dot indicates the approximate location of the foveal center. Top row: Eyes with small areas of multifocal GA. In the left image, the patient would experience a scotoma to the right. In the right image, the patient would experience a scotoma to the left, slightly above and slightly below fixation. Middle row: Eyes with horseshoe-shaped areas of atrophy. In the left image, the scotoma to the left would interfere the most, but there are also scotomas above and below fixation. In the image to the right, there is a scotoma near fixation just above fixation in the visual field space (inferior in the fundus image). There is also a scotoma below fixation. Bottom row: Eyes with macular ring scotomas. The image on the left is the fellow eye of the image just above it. This patient reported that he could read newsprint, but not newspaper headlines, because the headlines did not “fit” in the spared central area. The image on the right illustrates that even with a large area of GA, there is often persistent central sparing.
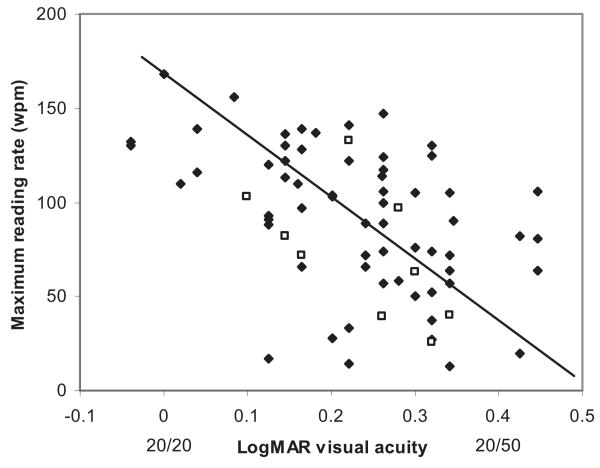
The baseline maximum reading rate as a function of the baseline visual acuity. Even within the range of good visual acuities included in this study, there is strong correlation between reading rate and visual acuity. The open squares are the eyes with the macular ring scotoma configuration of GA. The closed symbols are all the other eyes.
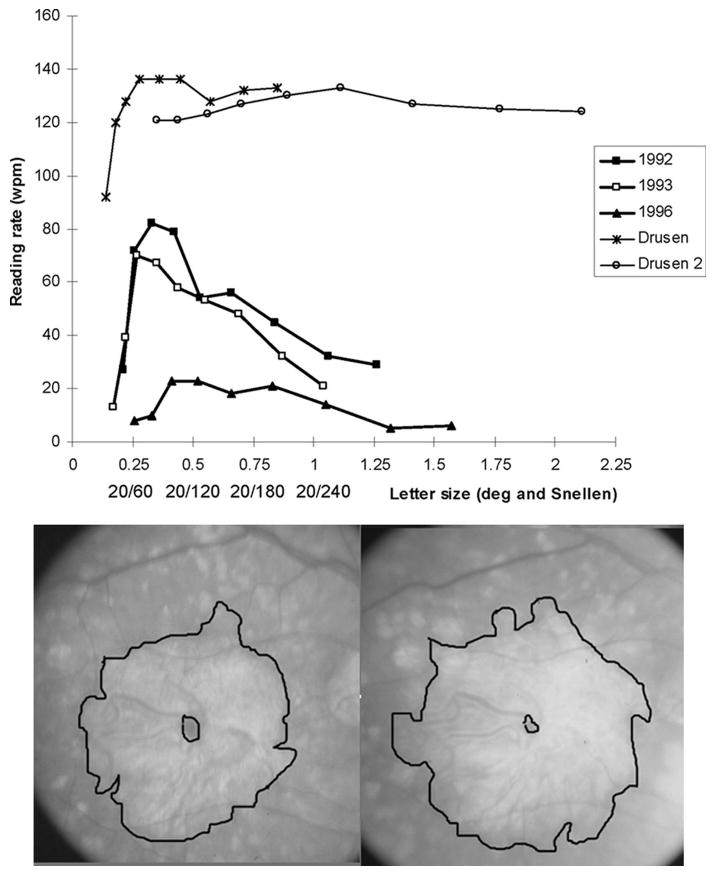
Top: Reading rate as a function of letter size. The findings of two eyes with drusen (all 11 eyes with drusen were similar) are shown at the top. For these eyes, once the maximum reading rate was attained, the reading rate remained essentially the same for increasing character size, out to the largest size tested (2 degrees). The longitudinal findings of one patient with a macular ring scotoma (bottom) are at the lower portion of the graph. At the baseline (1992), the maximum reading rate of 82 WPM was attained at 0.33 degrees, with a dramatic fall-off of the reading rate for larger letter sizes. One year later (1993), the results were similar, with a maximum reading rate of 70 WPM at 0.27 degrees, with a fall-off of the reading rate for larger letter sizes. At four years (1996), the maximum reading rate fell to 23 WPM without a sharp peak of the higher reading rate at the small letter size. Bottom: Fundus photographs of the eye with a macular ring scotoma, whose reading data are presented at the top of the figure. Left: In 1992, visual acuity was 0.14 logMAR (20/28). There was a small area of central sparing surrounded by a large area of GA and its corresponding dense scotoma. Right: In 1996, the visual acuity was 0.26 logMAR (20/36). There is still central sparing despite enlargement of the atrophy, but the central spared region was much smaller than in 1992.
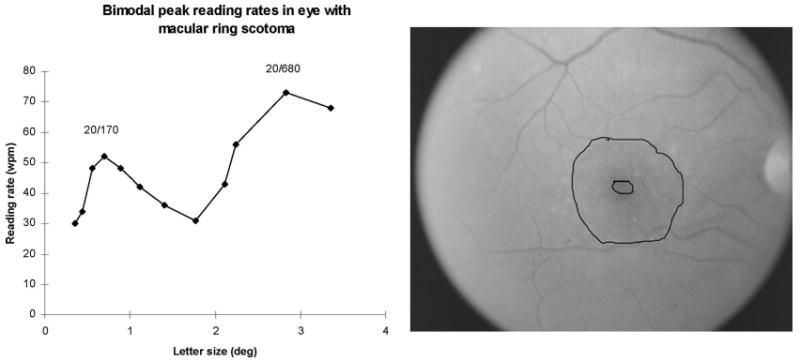
Bimodal reading rates in a patient in her early 50s with a macular ring scotoma from Stargardt disease. Visual acuity was 20/60. Left: The reading rate as a function of character size, tested here out to 3.5 degrees. There is a sharp peak reading rate of 52 WPM at the letter size of 0.70 degrees (20/170) and a second peak (and higher) reading rate of 73 WPM at the letter size 2.83 degrees (20/680). (The patients with good acuity in the GA study were not tested on letter sizes greater than 2 degrees.) Right: Fundus photograph of the eye whose data are presented to the left. There is a small central spared area surrounded by atrophy and dense scotoma.
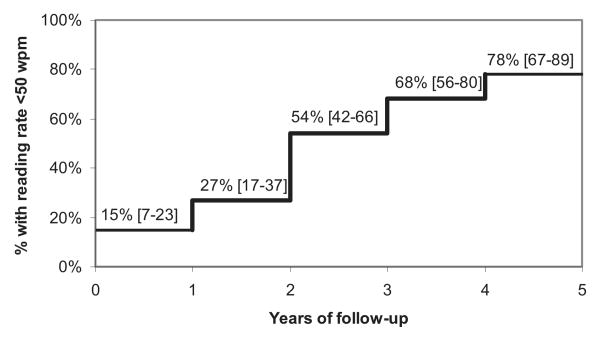
Kaplan-Meier survival analysis. The graph shows the percentage of eyes for each year of follow-up with a maximum reading rate fewer than 50 WPM. The 95% confidence limits are shown in brackets.
Similar articles
-
Reading newsprint but not headlines: pitfalls in measuring visual acuity and color vision in patients with bullseye maculopathy and other macular scotomas.Retin Cases Brief Rep. 2008 Winter;2(1):83-4. doi: 10.1097/IAE.0b013e31802fa25d. Retin Cases Brief Rep. 2008. PMID: 25389628
-
Fixation patterns and reading rates in eyes with central scotomas from advanced atrophic age-related macular degeneration and Stargardt disease.Ophthalmology. 1996 Sep;103(9):1458-66. doi: 10.1016/s0161-6420(96)30483-1. Ophthalmology. 1996. PMID: 8841306 Free PMC article.
-
Combined Fundus Autofluorescence and Near Infrared Reflectance as Prognostic Biomarkers for Visual Acuity in Foveal-Sparing Geographic Atrophy.Invest Ophthalmol Vis Sci. 2017 May 1;58(6):BIO61-BIO67. doi: 10.1167/iovs.16-21210. Invest Ophthalmol Vis Sci. 2017. PMID: 28475704 Clinical Trial.
-
The Progression of Geographic Atrophy Secondary to Age-Related Macular Degeneration.Ophthalmology. 2018 Mar;125(3):369-390. doi: 10.1016/j.ophtha.2017.08.038. Epub 2017 Oct 27. Ophthalmology. 2018. PMID: 29110945 Review.
-
The natural history of geographic atrophy, the advanced atrophic form of age-related macular degeneration.Mol Vis. 1999 Nov 3;5:25. Mol Vis. 1999. PMID: 10562649 Review.
Cited by
-
The Fovea-Protective Impact of Double-Layer Sign in Eyes With Foveal-Sparing Geographic Atrophy and Age-Related Macular Degeneration.Invest Ophthalmol Vis Sci. 2022 Oct 3;63(11):4. doi: 10.1167/iovs.63.11.4. Invest Ophthalmol Vis Sci. 2022. PMID: 36201174 Free PMC article.
-
Evaluation of Two Systems for Fundus-Controlled Scotopic and Mesopic Perimetry in Eye with Age-Related Macular Degeneration.Transl Vis Sci Technol. 2017 Jul 13;6(4):7. doi: 10.1167/tvst.6.4.7. eCollection 2017 Jul. Transl Vis Sci Technol. 2017. PMID: 28713647 Free PMC article.
-
Recent Advances in Imaging Macular Atrophy for Late-Stage Age-Related Macular Degeneration.Diagnostics (Basel). 2023 Dec 10;13(24):3635. doi: 10.3390/diagnostics13243635. Diagnostics (Basel). 2023. PMID: 38132220 Free PMC article. Review.
-
Living with Geographic Atrophy: An Ethnographic Study.Ophthalmol Ther. 2019 Mar;8(1):115-124. doi: 10.1007/s40123-019-0160-3. Epub 2019 Jan 31. Ophthalmol Ther. 2019. PMID: 30706242 Free PMC article.
-
Multimodal imaging and deep learning in geographic atrophy secondary to age-related macular degeneration.Acta Ophthalmol. 2023 Dec;101(8):881-890. doi: 10.1111/aos.15796. Acta Ophthalmol. 2023. PMID: 37933610 Free PMC article. Review.
References
-
- Fletcher DC, Schuchard RA. Preferred retinal loci: Relationship to macular scotomas in a low-vision population. Ophthalmology. 1997;104:632–638. - PubMed
-
- Gass JDM. Stereoscopic atlas of macular diseases. 4th. St. Louis, MO: Mosby; 1997.
-
- Green WR, Enger C. Age-related macular degeneration histopathologic studies: The 1992 Lorenz E. Zimmerman Lecture. Ophthalmology. 1993;100:1519–1535. - PubMed
-
- Hart WM, Burde RM. Three-dimensional topography of the central visual field: Sparing of foveal sensitivity in macular disease. Ophthalmology. 1983;90:1028–1038. - PubMed
-
- Lei H, Schuchard RA. Using two preferred retinal loci for different lighting conditions in patients with central scotomas. Investigative Ophthalmology & Vision Science. 1997;38:1812–1818. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources