

Initial Experience with Sildenafil, Bosentan, and Nitric Oxide for Pediatric Cardiomyopathy Patients with Elevated Pulmonary Vascular Resistance before and after Orthotopic Heart Transplantation
- PMID: 20224752
- PMCID: PMC2836130
- DOI: 10.1155/2010/656984
Initial Experience with Sildenafil, Bosentan, and Nitric Oxide for Pediatric Cardiomyopathy Patients with Elevated Pulmonary Vascular Resistance before and after Orthotopic Heart Transplantation
Abstract
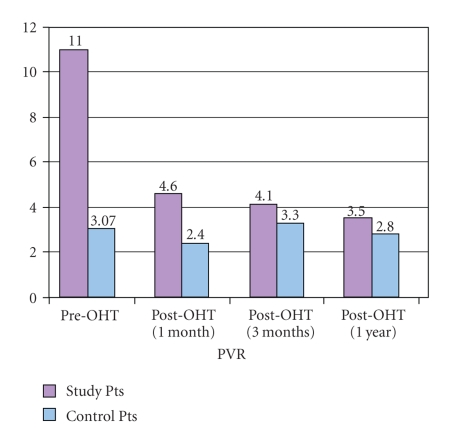
Background. Although pulmonary hypertension complicating dilated cardiomyopathy has been shown to be a significant risk factor for graft failure after heart transplantation, the upper limits of pulmonary vascular resistance (PVR) that would contraindicate pediatric heart transplantation are not known. Methods. A retrospective review of all pediatric orthotopic heart transplant (OHT) performed at our institution from 2002 to 2007 was performed. Seven patients with PVR > 6 Wood's units (WU) prior to transplant were compared pre- and postoperatively with 20 matched controls with PVR < 6 WU. All pulmonary vasodilator therapies used are described as well as outcomes during the first year posttransplant. Results. The mean PVR prior to transplantation in the 7 study cases was 11.0 +/- 4.6 (range 6-22) WU, compared to mean PVR of 3.07 +/- 0.9 WU (0.56-4.5) in the controls (P = .27 x 10(-6)). All patients with elevated PVR were treated pre-OHT with either Sildenafil or Bosentan. Post-OHT, case patients received a combination of sildenafil, iloprost, and inhaled nitric oxide. All 7 case patients survived one year post-OHT, and there was no statistical difference between cases and controls for hospital stay, rejection/readmissions, or graft right ventricular failure. Mean PVR in the cases at one and three months post-OHT was not significantly different between the two groups. Only one of the cases required prolonged treatment with iloprost after OHT. Conclusions. A PVR above 6 WU should not be an absolute contraindication to heart transplantation in children.
References
-
- Chen JM, Levin HR, Michler RE, Prusmack CJ, Rose EA, Aaronson KD. Reevaluating the significance of pulmonary hypertension before cardiac transplantation: determination of optimal thresholds and quantification of the effect of reversibility on perioperative mortality. Journal of Thoracic and Cardiovascular Surgery. 1997;114(4):627–634. - PubMed
-
- Kirklin JK, Naftel DC, Kirklin JW, Blackstone EH, White-Williams C, Bourge RC. Pulmonary vascular resistance and the risk of heart transplantation. Journal of Heart Transplantation. 1988;7(5):331–336. - PubMed
-
- Delgado JF, Gomez-Sanchez MA, Saenz de la Calzada C, et al. Impact of mild pulmonary hypertension on mortality and pulmonary artery pressure profile after heart transplantation. Journal of Heart and Lung Transplantation. 2001;20(9):942–948. - PubMed
-
- Chang PP, Longenecker JC, Wang N-Y, et al. Mild vs severe pulmonary hypertension before heart transplantation: different effects on posttransplantation pulmonary hypertension and mortality. Journal of Heart and Lung Transplantation. 2005;24(8):998–1007. - PubMed
-
- Costard-Jackle A, Fowler MB. Influence of preoperative pulmonary artery pressure on mortality after heart transplantation: testing of potential reversibility of pulmonary hypertension with nitroprusside is useful in defining a high risk group. Journal of the American College of Cardiology. 1992;19(1):48–54. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
