

Genital tuberculosis as the cause of tuboovarian abscess in an immunosuppressed patient
- PMID: 20224814
- PMCID: PMC2834956
- DOI: 10.1155/2009/745060
Genital tuberculosis as the cause of tuboovarian abscess in an immunosuppressed patient
Abstract
Background: Although tuberculosis (TB) is a major health problem worldwide, primary extrapulmonary tuberculosis (EPTB), and in particular female genital tract infection, remains a rare event.
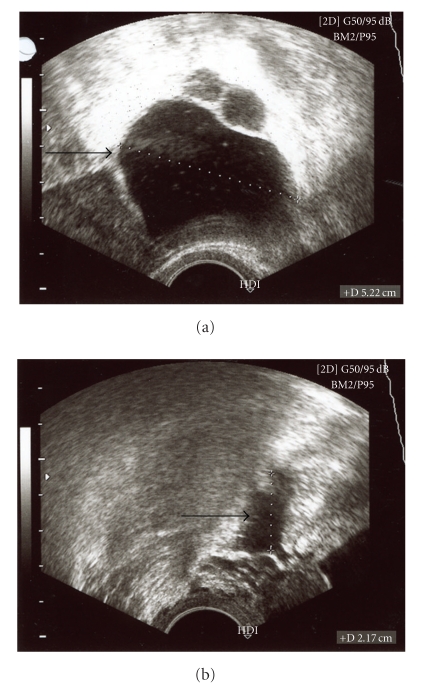
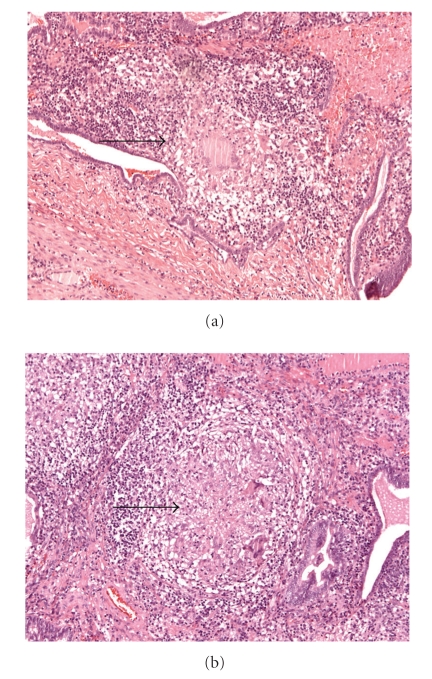
Case report: A 35-year-old human immunodeficiency virus (HIV) seropositive woman of African descent with lower abdominal pain and fever of two days duration underwent surgery due to left adnexal mass suggesting pelvic inflammatory disease. The surgical situs showed a four quadrant peritonitis, consistent with the clinical symptoms of the patient, provoked by a tuboovarian abscess (TOA) on the left side. All routine diagnostic procedures failed to determine the causative organism/pathogen of the infection. Histopathological evaluation identified a necrotic granulomatous salpingitis and specific PCR analysis corroborated Mycobacterium tuberculosis (M. Tb). Consequently, antituberculotic therapy was provided.
Conclusion: In the differential diagnosis of pelvic inflammatory disease, internal genital tuberculosis should be considered. Moreover, physicians should consider tuberculous infections early in the work-up of patients when immunosuppressive conditions are present.
Figures
Similar articles
-
Computed tomographic features of tuboovarian abscess.J Reprod Med. 2005 Mar;50(3):203-8. J Reprod Med. 2005. PMID: 15841934
-
Pathogenesis, diagnosis, and management of severe pelvic inflammatory disease and tuboovarian abscess.Clin Obstet Gynecol. 2012 Dec;55(4):893-903. doi: 10.1097/GRF.0b013e3182714681. Clin Obstet Gynecol. 2012. PMID: 23090458 Review.
-
Ruptured tuboovarian abscess causing peritonitis in a postmenopausal woman. A difficult diagnosis on imaging.JBR-BTR. 2003 Mar-Apr;86(2):72-3. JBR-BTR. 2003. PMID: 12839418
-
Pasteurella multocida bacteremia and tuboovarian abscess.Obstet Gynecol. 2005 Nov;106(5 Pt 2):1220-2. doi: 10.1097/01.AOG.0000164063.24495.75. Obstet Gynecol. 2005. PMID: 16260579
-
Tubo-ovarian abscess caused by Clostridioides difficile after eight months of surgery: Case report and review of extraintestinal abdominal abscess cases.J Infect Chemother. 2025 Jan;31(1):102432. doi: 10.1016/j.jiac.2024.05.012. Epub 2024 Jun 1. J Infect Chemother. 2025. PMID: 38825001 Review.
Cited by
-
Typical and unusual cases of female genital tuberculosis.IDCases. 2014 Oct 31;1(4):92-4. doi: 10.1016/j.idcr.2014.10.001. eCollection 2014. IDCases. 2014. PMID: 26839784 Free PMC article.
-
An extremely rare case of tubo-ovarian abscesses involving corynebacterium striatum as causative agent.BMC Infect Dis. 2016 Sep 29;16(1):527. doi: 10.1186/s12879-016-1860-0. BMC Infect Dis. 2016. PMID: 27686475 Free PMC article.
-
Current Advances in Lipid-Based Drug Delivery Systems as Nanocarriers for the Management of Female Genital Tuberculosis.Cureus. 2024 Nov 25;16(11):e74452. doi: 10.7759/cureus.74452. eCollection 2024 Nov. Cureus. 2024. PMID: 39726465 Free PMC article. Review.
-
Genital Tuberculosis and Serous Cystadenoma in a 58-Year-Old Female With Rheumatoid Arthritis and Sjögren's Syndrome: A Case Report.Case Rep Rheumatol. 2025 May 6;2025:9372058. doi: 10.1155/crrh/9372058. eCollection 2025. Case Rep Rheumatol. 2025. PMID: 40365452 Free PMC article.
-
Large bilateral tubercular pyosalpinx in a young woman with genitourinary malformation: a case report.J Med Case Rep. 2014 Jun 3;8:176. doi: 10.1186/1752-1947-8-176. J Med Case Rep. 2014. PMID: 24894269 Free PMC article.
References
-
- Haggerty CL. Evidence for a role of Mycoplasma genitalium in pelvic inflammatory disease. Current Opinion in Infectious Diseases. 2008;21(1):65–69. - PubMed
-
- Corbett EL, Watt CJ, Walker N, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Archives of Internal Medicine. 2003;163(9):1009–1021. - PubMed
-
- Hsieh H-C, Lu P-L, Chen Y-H, et al. Genitourinary tuberculosis in a medical center in southern Taiwan: an eleven-year experience. Journal of Microbiology, Immunology and Infection. 2006;39(5):408–413. - PubMed
-
- Letvin NL, Walker BD. Immunopathogenesis and immunotherapy in AIDS virus infections. Nature Medicine. 2003;9(7):861–866. - PubMed
-
- Sebitloane MH. HIV and gynaecological infections. Best Practice and Research: Clinical Obstetrics and Gynaecology. 2005;19(2):231–241. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
