

The course of the superficial peroneal nerve in relation to the ankle position: anatomical study with ankle arthroscopic implications
- PMID: 20224993
- PMCID: PMC2855034
- DOI: 10.1007/s00167-010-1099-z
The course of the superficial peroneal nerve in relation to the ankle position: anatomical study with ankle arthroscopic implications
Abstract
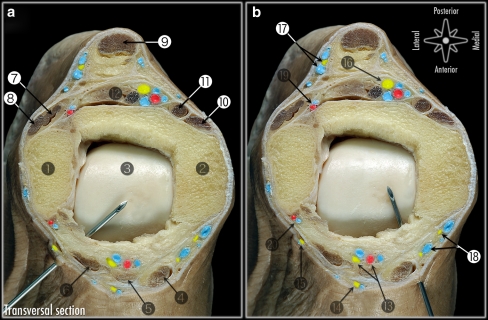
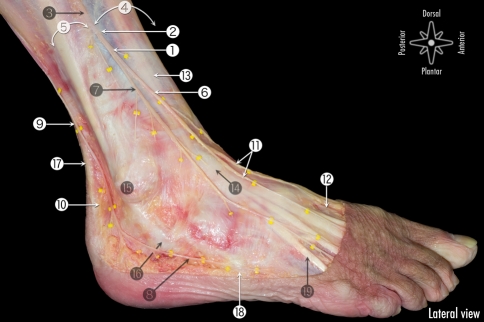
Despite the fact that the superficial peroneal nerve is the only nerve in the human body that can be made visible; iatrogenic damage to this nerve is the most frequently reported complication in anterior ankle arthroscopy. One of the methods to visualize the nerve is combined ankle plantar flexion and inversion. In the majority of cases, the superficial peroneal nerve can be made visible. The portals for anterior ankle arthroscopy are however created with the ankle in the neutral or slightly dorsiflexed position and not in combined plantar flexion and inversion. The purpose of this study was to undertake an anatomical study to the course of the superficial peroneal nerve in different positions of the foot and ankle. We hypothesize that the anatomical localization of the superficial peroneal nerve changes with different foot and ankle positions. In ten fresh frozen ankle specimens, a window, only affecting the skin, was made at the level of the anterolateral portal for anterior ankle arthroscopy in order to directly visualize the superficial peroneal nerve, or if divided, its terminal branches. Nerve movement was assessed from combined 10 degrees plantar flexion and inversion to 5 degrees dorsiflexion, standardized by the Telos stress device. Also for the 4th toe flexion, flexion of all the toes and for skin tensioning possible nerve movement was determined. The mean superficial peroneal nerve movement was 2.4 mm to the lateral side when the ankle was moved from 10 degrees plantar flexion and inversion to the neutral ankle position and 3.6 mm to the lateral side from 10 degrees plantar flexion and inversion to 5 degrees dorsiflexion. Both displacements were significant (P < 0.01). The nerve consistently moves lateral when the ankle is manoeuvred from combined plantar flexion and inversion to the neutral or dorsiflexed position. If visible, it is therefore advised to create the anterolateral portal medial from the preoperative marking, in order to prevent iatrogenic damage to the superficial peroneal nerve.
Figures


References
-
- Adkison DP, Bosse MJ, Gaccione DR, et al. Anatomical variations in the course of the superficial peroneal nerve. J Bone Joint Surg Am. 1991;73:112–114. - PubMed
-
- Amendola A, Petrik J, Webster-Bogaert S. Ankle arthroscopy: outcome in 79 consecutive patients. Arthroscopy. 1996;12:565–573. - PubMed
-
- Barber FA, Britt BT, Ratliff HW, et al. Arthroscopic surgery of the ankle. Orthop Rev. 1988;17:446–451. - PubMed
-
- Barber FA, Click J, Britt BT. Complications of ankle arthroscopy. Foot Ankle. 1990;10:263–266. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
