

High-frequency electroencephalographic oscillations correlate with outcome of epilepsy surgery
- PMID: 20225281
- PMCID: PMC3769290
- DOI: 10.1002/ana.21847
High-frequency electroencephalographic oscillations correlate with outcome of epilepsy surgery
Abstract
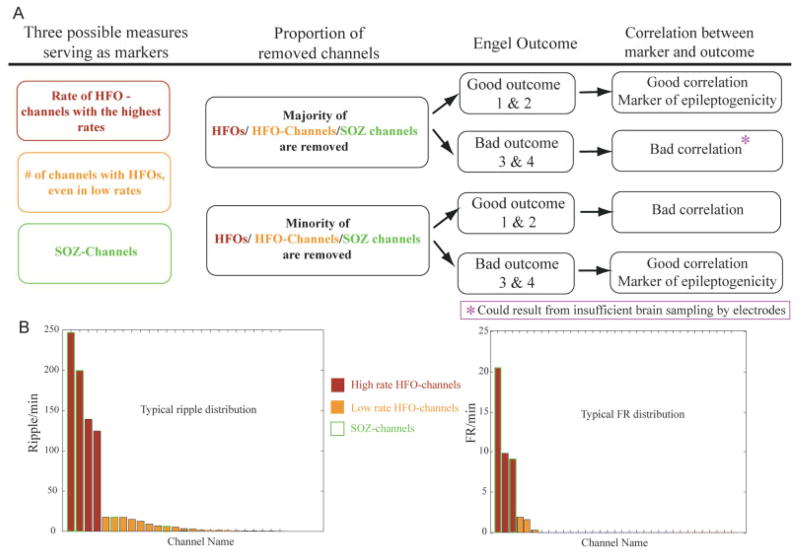
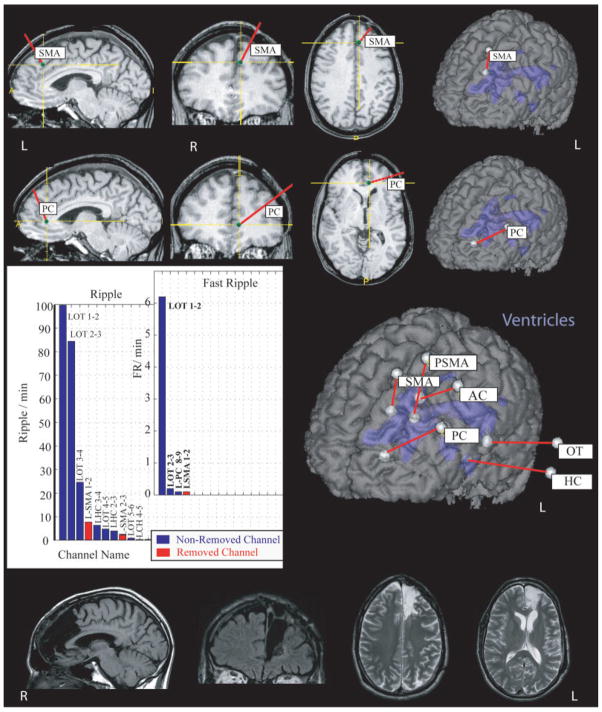
Objective: High-frequency oscillations (HFOs) in the intracerebral electroencephalogram (EEG) have been linked to the seizure onset zone (SOZ). We investigated whether HFOs can delineate epileptogenic areas even outside the SOZ by correlating the resection of HFO-generating areas with surgical outcome.
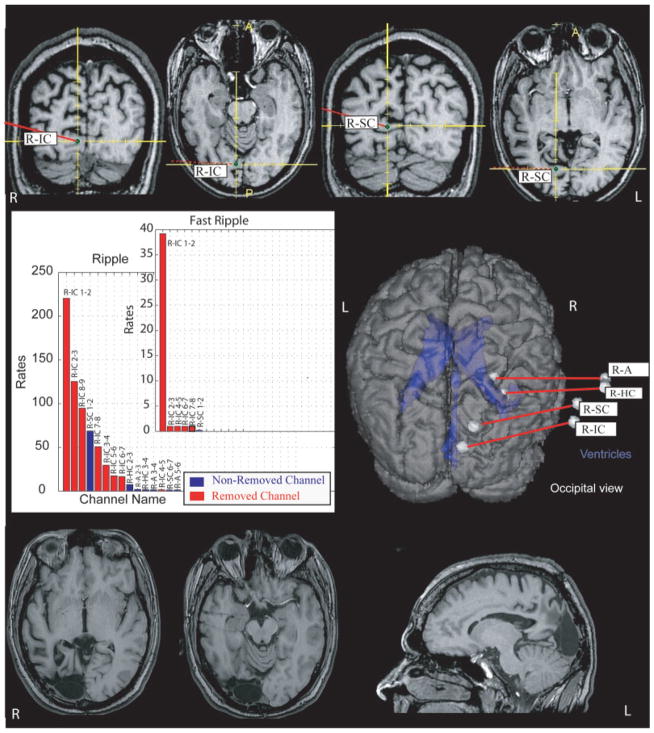
Methods: Twenty patients who underwent a surgical resection for medically intractable epilepsy were studied. All had presurgical intracerebral EEG (500Hz filter and 2,000Hz sampling rate), at least 12-month postsurgical follow-up, and a postsurgical magnetic resonance imaging (MRI). HFOs (ripples, 80-250Hz; fast ripples, >250Hz) were identified visually during 5 to 10 minutes of slow-wave sleep. Rates and extent of HFOs and interictal spikes in resected versus nonresected areas, assessed on postsurgical MRIs, were compared with surgical outcome (Engel's classification). We also evaluated the predictive value of removing the SOZ in terms of surgical outcome.
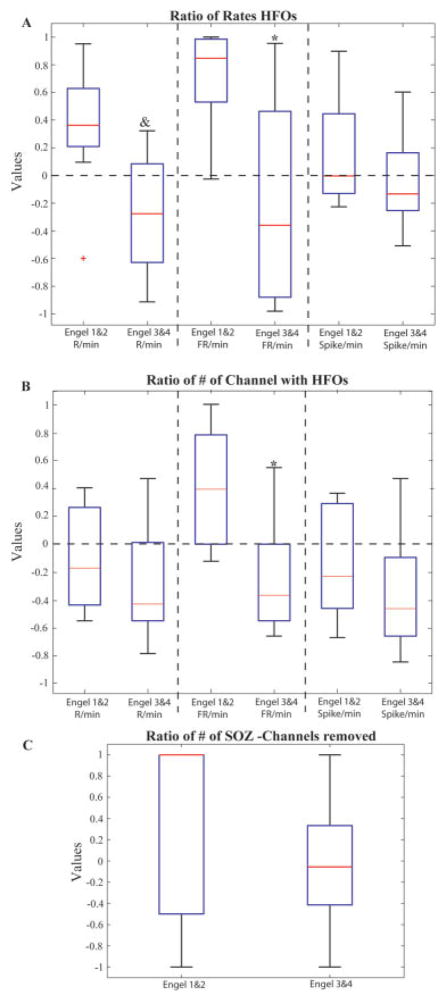
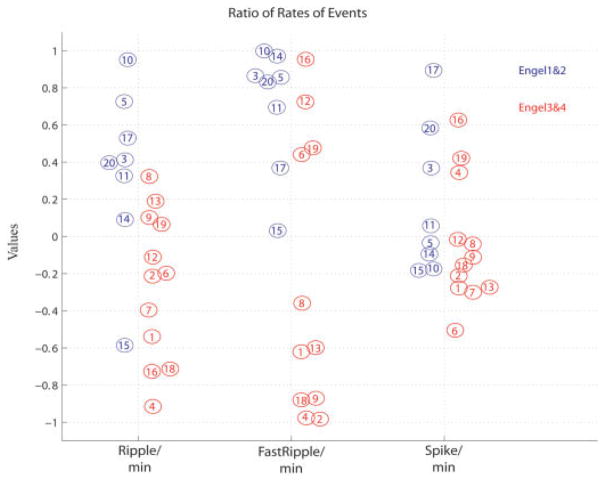
Results: The mean duration of follow-up was 22.7 months. Eight patients had good (Engel classes 1 and 2) and 12 poor (classes 3 and 4) surgical outcomes. Patients with a good outcome had a significantly larger proportion of HFO-generating areas removed than patients with a poor outcome. No such difference was seen for spike-generating regions or the SOZ.
Interpretation: The correlation between removal of HFO-generating areas and good surgical outcome indicates that HFOs could be used as a marker of epileptogenicity and may be more accurate than spike-generating areas or the SOZ. In patients in whom the majority of HFO-generating tissue remained, a poor surgical outcome occurred.
Figures
References
-
- Schuele SU, Lüders HO. Intractable epilepsy: management and therapeutic alternatives. Lancet Neurol. 2008;7:514–524. - PubMed
-
- Diehl B, Lüders HO. Temporal lobe epilepsy: when are invasive recordings needed? Epilepsia. 2000;41(suppl 3):61–74. - PubMed
-
- Rosenow F, Lüders H. Presurgical evaluation of epilepsy. Brain. 2001;124(pt 9):1683–1700. - PubMed
-
- Boling W, Aghakhani Y, Andermann F, Sziklas V, Olivier A. Surgical treatment of independent bitemporal lobe epilepsy defined by invasive recordings. J Neurol Neurosurg Psychiatry. 2009;80:533–538. - PubMed
-
- Prasad A, Pacia SV, Vazquez B, et al. Extent of ictal origin in mesial temporal sclerosis patients monitored with subdural intracranial electrodes predicts outcome. Clin Neurophysiol. 2003;20:243–248. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
