

Coverage optimized planning: probabilistic treatment planning based on dose coverage histogram criteria
- PMID: 20229863
- PMCID: PMC2816984
- DOI: 10.1118/1.3273063
Coverage optimized planning: probabilistic treatment planning based on dose coverage histogram criteria
Abstract
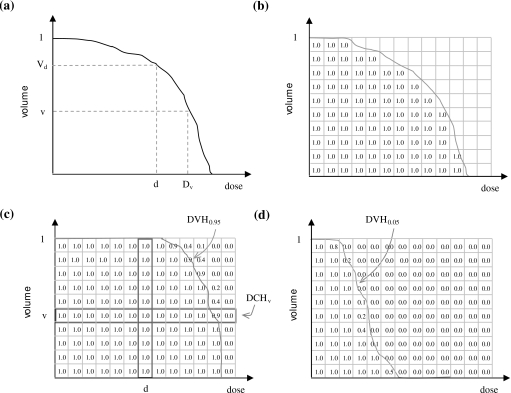
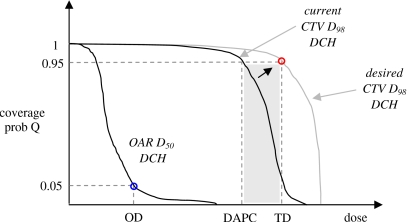
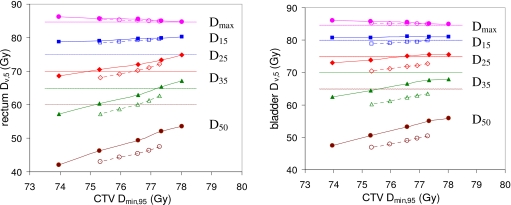
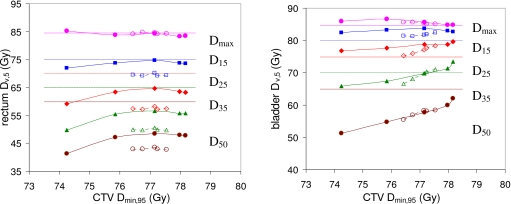
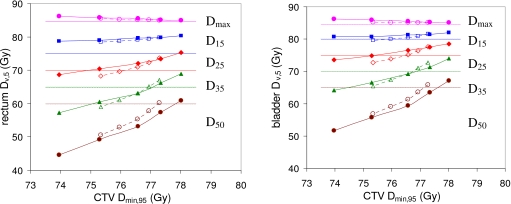
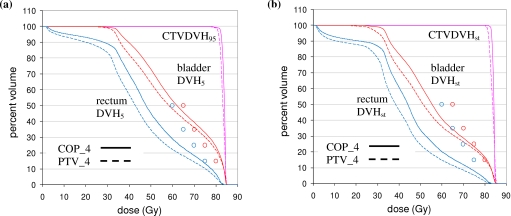
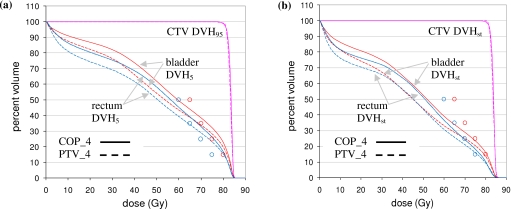
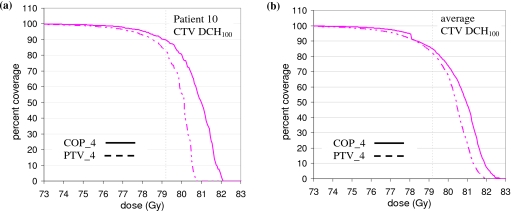
This work (i) proposes a probabilistic treatment planning framework, termed coverage optimized planning (COP), based on dose coverage histogram (DCH) criteria; (ii) describes a concrete proof-of-concept implementation of COP within the PINNACLE treatment planning system; and (iii) for a set of 28 prostate anatomies, compares COP plans generated with this implementation to traditional PTV-based plans generated with planning criteria approximating those in the high dose arm of the Radiation Therapy Oncology Group 0126 protocol. Let Dv denote the dose delivered to fractional volume v of a structure. In conventional intensity modulated radiation therapy planning, Dv has a unique value derived from the static (planned) dose distribution. In the presence of geometric uncertainties (e.g., setup errors) Dv assumes a range of values. The DCH is the complementary cumulative distribution function of D(v+). DCHs are similar to dose volume histograms (DVHs). Whereas a DVH plots volume v versus dose D, a DCH plots coverage probability Q versus D. For a given patient, Q is the probability (i.e., percentage of geometric uncertainties) for which the realized value of Dv exceeds D. PTV-based treatment plans can be converted to COP plans by replacing DVH optimization criteria with corresponding DCH criteria. In this approach, PTVs and planning organ at risk volumes are discarded, and DCH criteria are instead applied directly to clinical target volumes (CTVs) or organs at risk (OARs). Plans are optimized using a similar strategy as for DVH criteria. The specific implementation is described. COP was found to produce better plans than standard PTV-based plans, in the following sense. While target OAR dose tradeoff curves were equivalent to those for PTV-based plans, COP plans were able to exploit slack in OAR doses, i.e., cases where OAR doses were below their optimization limits, to increase target coverage. Specifically, because COP plans were not constrained by a predefined PTV, they were able to provide wider dosimetric margins around the CTV, by pushing OAR doses up to, but not beyond, their optimization limits. COP plans demonstrated improved target coverage when averaged over all 28 prostate anatomies, indicating that the COP approach can provide benefits for many patients. However, the degree to which slack OAR doses can be exploited to increase target coverage will vary according to the individual patient anatomy. The proof-of-concept COP implementation investigated here utilized a probabilistic DCH criteria only for the CTV minimum dose criterion. All other optimization criteria were conventional DVH criteria. In a mature COP implementation, all optimization criteria will be DCH criteria, enabling direct planning control over probabilistic dose distributions. Further research is necessary to determine the benefits of COP planning, in terms of tumor control probability and/or normal tissue complication probabilities.
Figures
Similar articles
-
Dose-shaping using targeted sparse optimization.Med Phys. 2013 Jul;40(7):071711. doi: 10.1118/1.4808363. Med Phys. 2013. PMID: 23822415
-
A new method of incorporating systematic uncertainties in intensity-modulated radiotherapy optimization.Med Phys. 2005 Aug;32(8):2567-79. doi: 10.1118/1.1954161. Med Phys. 2005. PMID: 16193787
-
Evaluation of dosimetric margins in prostate IMRT treatment plans.Med Phys. 2008 Feb;35(2):569-75. doi: 10.1118/1.2826558. Med Phys. 2008. PMID: 18383678 Free PMC article.
-
Robust Proton Treatment Planning: Physical and Biological Optimization.Semin Radiat Oncol. 2018 Apr;28(2):88-96. doi: 10.1016/j.semradonc.2017.11.005. Semin Radiat Oncol. 2018. PMID: 29735195 Free PMC article. Review.
-
Optimized planning using physical objectives and constraints.Semin Radiat Oncol. 1999 Jan;9(1):20-34. doi: 10.1016/s1053-4296(99)80052-6. Semin Radiat Oncol. 1999. PMID: 10196396 Review.
Cited by
-
Classifying geometric variability by dominant eigenmodes of deformation in regressing tumours during active breath-hold lung cancer radiotherapy.Phys Med Biol. 2012 Jan 21;57(2):395-413. doi: 10.1088/0031-9155/57/2/395. Epub 2011 Dec 15. Phys Med Biol. 2012. PMID: 22172998 Free PMC article.
-
Comparisons of treatment optimization directly incorporating systematic patient setup uncertainty with a margin-based approach.Med Phys. 2012 Feb;39(2):1102-11. doi: 10.1118/1.3679856. Med Phys. 2012. PMID: 22320820 Free PMC article.
-
Clinical adequacy assessment of autocontours for prostate IMRT with meaningful endpoints.Med Phys. 2017 Apr;44(4):1525-1537. doi: 10.1002/mp.12158. Med Phys. 2017. PMID: 28196288 Free PMC article.
-
Novel adaptive beam-dependent margins for additional OAR sparing.Phys Med Biol. 2018 Oct 29;63(21):215019. doi: 10.1088/1361-6560/aae658. Phys Med Biol. 2018. PMID: 30372420 Free PMC article.
-
Robustness Analysis for External Beam Radiation Therapy Treatment Plans: Describing Uncertainty Scenarios and Reporting Their Dosimetric Consequences.Pract Radiat Oncol. 2019 Jul-Aug;9(4):200-207. doi: 10.1016/j.prro.2018.12.002. Epub 2018 Dec 15. Pract Radiat Oncol. 2019. PMID: 30562614 Free PMC article. Review.
References
-
- Dušan M., “Verification and correction of geometrical uncertainties in conformal radiotherapy,” Arch. Oncol. ZZZZZZ 13(3–4), 140–144 (2005).10.2298/AOO0504140M - DOI
-
- International Commission on Radiation Units and Measurements, “Prescribing, recording and reporting photon beam therapy,” ICRU Report No. 50 (ICRU Publications, Bethesda, MD, 1994).
-
- International Commission on Radiation Units and Measurements, “Prescribing, recording and reporting photon beam therapy (Supplement to ICRU Report No. 50),” ICRU Report No. 62 (ICRU Publications, Bethesda, MD, 2000).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
