

Infections of respiratory or abdominal origin in ICU patients: what are the differences?
- PMID: 20230620
- PMCID: PMC2887138
- DOI: 10.1186/cc8909
Infections of respiratory or abdominal origin in ICU patients: what are the differences?
Abstract
Introduction: There are few data related to the effects of different sources of infection on outcome. We used the Sepsis Occurrence in Acutely ill Patients (SOAP) database to investigate differences in the impact of respiratory tract and abdominal sites of infection on organ failure and survival.
Methods: The SOAP study was a cohort, multicenter, observational study which included data from all adult patients admitted to one of 198 participating intensive care units (ICUs) from 24 European countries during the study period. In this substudy, patients were divided into two groups depending on whether, on admission, they had abdominal infection but no respiratory infection or respiratory infection but no abdominal infection. The two groups were compared with respect to patient and infection-related characteristics, organ failure patterns, and outcomes.
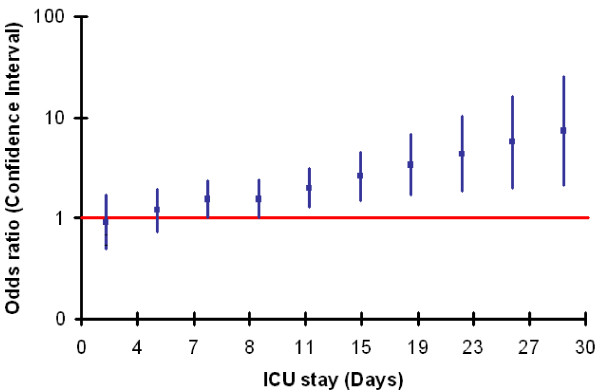
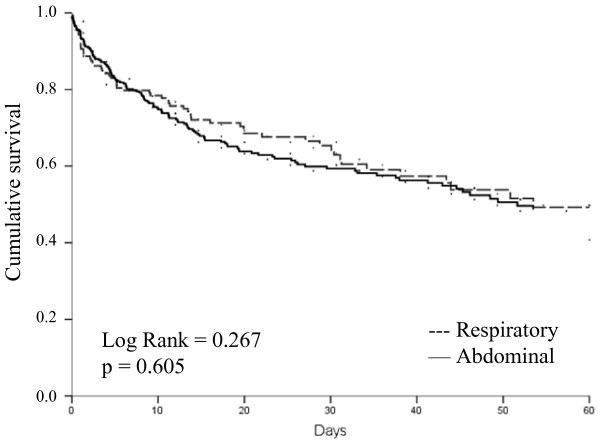
Results: Of the 3,147 patients in the SOAP database, 777 (25%) patients had sepsis on ICU admission; 162 (21%) had abdominal infection without concurrent respiratory infection and 380 (49%) had respiratory infection without concurrent abdominal infection. Age, sex, and severity scores were similar in the two groups. On admission, septic shock was more common in patients with abdominal infection (40.1% vs. 29.5%, P = 0.016) who were also more likely to have early coagulation failure (17.3% vs. 9.5%, P = 0.01) and acute renal failure (38.3% vs. 29.5%, P = 0.045). In contrast, patients with respiratory infection were more likely to have early neurological failure (30.5% vs. 9.9%, P < 0.001). The median length of ICU stay was the same in the two groups, but the median length of hospital stay was longer in patients with abdominal than in those with respiratory infection (27 vs. 20 days, P = 0.02). ICU (29%) and hospital (38%) mortality rates were identical in the two groups.
Conclusions: There are important differences in patient profiles related to the site of infection; however, mortality rates in these two groups of patients are identical.
Figures
References
-
- Vincent JL, Rello J, Marshall J, Silva E, Anzueto A, Martin CD, Moreno R, Lipman J, Gomersall C, Sakr Y, Reinhart K. EPIC II Groups of Investigators. International study of the prevalence and outcomes of infection in intensive care units. JAMA. 2009;302:2323–2329. doi: 10.1001/jama.2009.1754. - DOI - PubMed
-
- Alberti C, Brun-Buisson C, Burchardi H, Martin C, Goodman S, Artigas A, Sicignano A, Palazzo M, Moreno R, Boulme R, Lepage E, Le Gall R. Epidemiology of sepsis and infection in ICU patients from an international multicentre cohort study. Intensive Care Med. 2002;28:108–121. doi: 10.1007/s00134-001-1143-z. - DOI - PubMed
-
- Malacarne P, Langer M, Nascimben E, Moro ML, Giudici D, Lampati L, Bertolini G. Building a continuous multicenter infection surveillance system in the intensive care unit: findings from the initial data set of 9,493 patients from 71 Italian intensive care units. Crit Care Med. 2008;36:1105–1113. doi: 10.1097/CCM.0b013e318169ed30. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
