

Minimal residual disease detection by flow cytometry in adult T-cell leukemia/lymphoma
- PMID: 20231613
- PMCID: PMC7596844
- DOI: 10.1309/AJCPS1K0OHLJYWWV
Minimal residual disease detection by flow cytometry in adult T-cell leukemia/lymphoma
Abstract
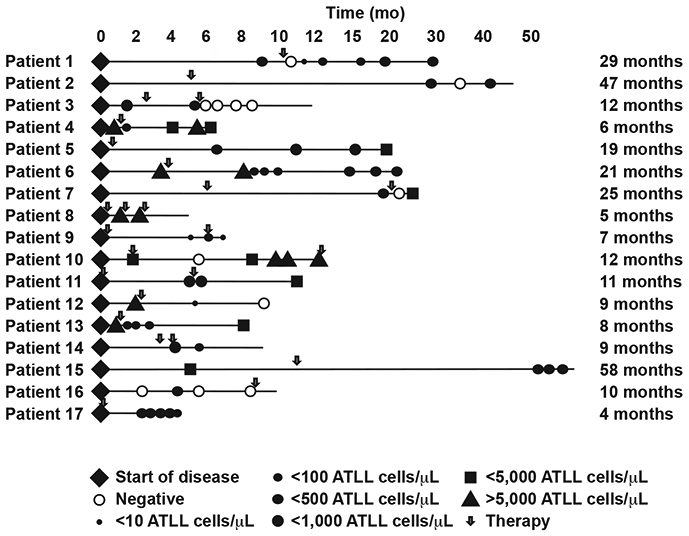
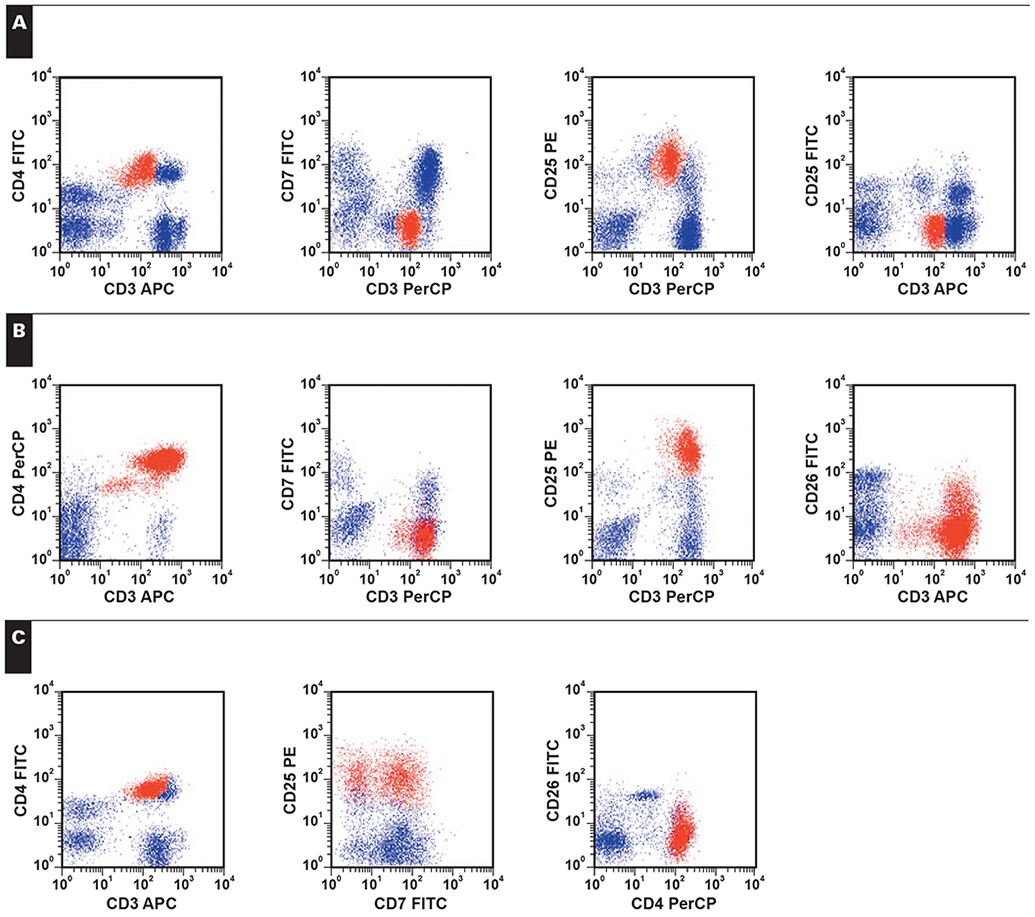
Little information exists regarding the detection of minimal residual disease (MRD) in adult T-cell leukemia/lymphoma (ATLL). We evaluated 75 peripheral blood samples from 17 ATLL cases using flow cytometry (FC); 50 of the samples were concurrently evaluated by polymerase chain reaction (PCR) for clonal T-cell receptor gamma chain (TRG) gene rearrangement and the presence of human T-cell lymphotropic virus-1 proviral sequences. Residual ATLL cells were identified using a multiparametric approach to identify aberrant T-cell immunophenotypes. Malignant T cells were CD4+, CD3 dim+, CD26-, CD25 bright, CD7+, and CD27+, with occasional dim expression of CD2 or CD5. FC exhibited a high sensitivity, detecting as few as 0.29% ATLL cells/WBC (4.9 cells/microL) in the peripheral blood. PCR for TRG gene rearrangement was slightly more sensitive, and FC and PCR complemented each other in detecting MRD. In 2 patients, there was complete remission; 4 patients had disease refractory to therapy, and 3 died; 11 others had persistent disease with variable numbers of ATLL cells in the peripheral blood. Higher levels of ATLL cells appeared to correlate with disease severity. FC detection of aberrant T cells permits sensitive and quantitative monitoring of MRD in ATLL.
Figures
Similar articles
-
Adult T-cell leukemia/lymphoma (ATLL): report of two fully documented Hellenic patients.Leuk Lymphoma. 2004 Apr;45(4):715-21. doi: 10.1080/1042819032000140960. Leuk Lymphoma. 2004. PMID: 15160945
-
[Clinicopathological characteristics of adult T cell leukemia/lymphoma].Zhonghua Bing Li Xue Za Zhi. 2019 Jan 8;48(1):11-16. doi: 10.3760/cma.j.issn.0529-5807.2019.01.003. Zhonghua Bing Li Xue Za Zhi. 2019. PMID: 30641639 Review. Chinese.
-
BIOMED-1 concerted action report: flow cytometric characterization of CD7+ cell subsets in normal bone marrow as a basis for the diagnosis and follow-up of T cell acute lymphoblastic leukemia (T-ALL).Leukemia. 2000 May;14(5):816-25. doi: 10.1038/sj.leu.2401741. Leukemia. 2000. PMID: 10803512
-
CD4 and CD8 double-negative adult T-cell leukemia/lymphoma with monomorphic cells expressing CD99: a diagnostic challenge in a country non-endemic for human T-cell leukemia virus.Pathol Int. 2013 Feb;63(2):132-7. doi: 10.1111/pin.12040. Pathol Int. 2013. PMID: 23464972
-
Molecular Pathology of Adult T-Cell Leukemia/Lymphoma.Oncology. 2015;89 Suppl 1:7-15. doi: 10.1159/000431058. Epub 2015 Nov 10. Oncology. 2015. PMID: 26550829 Review.
Cited by
-
Flow cytometric profiles with CD7 and CADM1 in CD4+ T cells are promising indicators for prognosis of aggressive ATL.Blood Adv. 2024 Jul 23;8(14):3760-3770. doi: 10.1182/bloodadvances.2024013089. Blood Adv. 2024. PMID: 38820467 Free PMC article.
-
Flow cytometric immunophenotypic assessment of T-cell clonality by Vβ repertoire analysis: detection of T-cell clonality at diagnosis and monitoring of minimal residual disease following therapy.Am J Clin Pathol. 2011 Jun;135(6):890-900. doi: 10.1309/AJCPV2D1DDSGJDBW. Am J Clin Pathol. 2011. PMID: 21571962 Free PMC article.
-
CD27 expression and its association with clinical outcome in children and adults with pro-B acute lymphoblastic leukemia.Blood Cancer J. 2017 Jun 23;7(6):e575. doi: 10.1038/bcj.2017.55. Blood Cancer J. 2017. PMID: 28649984 Free PMC article. No abstract available.
-
Role of stem-like cells in chemotherapy resistance and relapse in pediatric T-cell acute lymphoblastic leukemia.Nat Commun. 2025 Jun 27;16(1):5413. doi: 10.1038/s41467-025-61222-1. Nat Commun. 2025. PMID: 40579412 Free PMC article.
-
Updates in lymph node and skin pathology of adult T-cell leukemia/lymphoma, biomarkers, and beyond.Semin Diagn Pathol. 2020 Jan;37(1):1-10. doi: 10.1053/j.semdp.2019.12.006. Epub 2019 Dec 20. Semin Diagn Pathol. 2020. PMID: 31889601 Free PMC article. Review.
References
-
- Manns A, Hisada M, La Grenade L. Human T-lymphotropic virus type I infection. Lancet. 1999;353:1951–1958. - PubMed
-
- Siegel RS, Gartenhaus RB, Kuzel TM. Human T-cell lymphotropic-I–leukemia/lymphoma. Curr Treat Options Oncol. 2001;2:291–300. - PubMed
-
- Murphy EL, Hanchard B, Figueroa JP, et al. Modelling the risk of adult T-cell leukemia/lymphoma in persons infected with human T-lymphotropic virus type I. Int J Cancer. 1989;43:250–253. - PubMed
-
- Yamaguchi K Human T-lymphotropic virus type I in Japan. Lancet. 1994;343:213–216. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
