

Beta-blocker efficacy in high-risk patients with the congenital long-QT syndrome types 1 and 2: implications for patient management
- PMID: 20233272
- PMCID: PMC4005824
- DOI: 10.1111/j.1540-8167.2010.01737.x
Beta-blocker efficacy in high-risk patients with the congenital long-QT syndrome types 1 and 2: implications for patient management
Abstract
Background: Beta-blockers are the mainstay therapy in patients with the congenital long-QT syndrome (LQTS) types 1 and 2. However, limited data exist regarding the efficacy and limitations of this form of medical management within high-risk subsets of these populations.
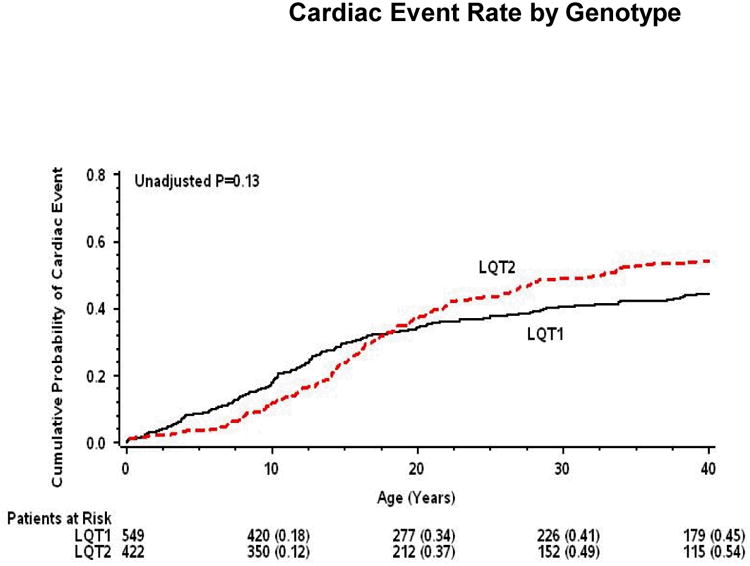
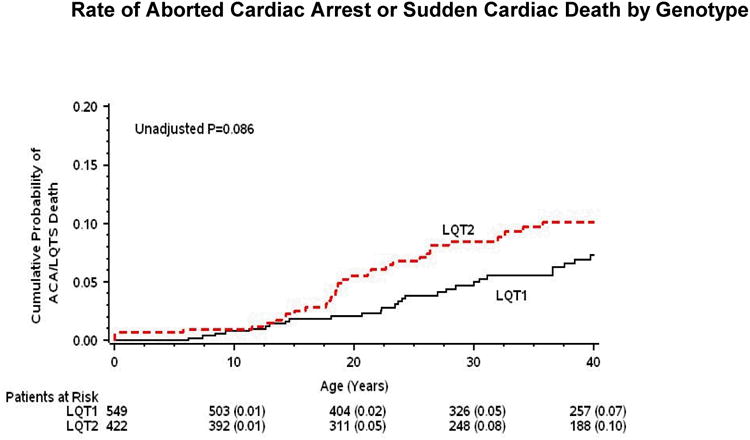
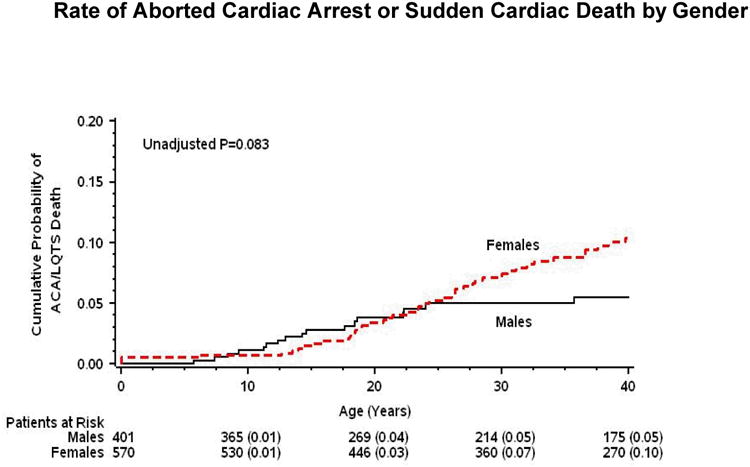
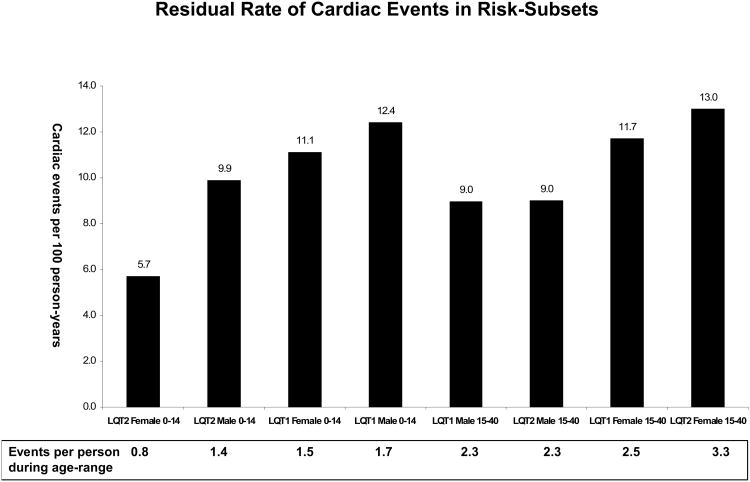
Methods and results: Multivariate analysis was carried out to identify age-related gender- and genotype-specific risk factors for cardiac events (comprising syncope, aborted cardiac arrest [ACA] or sudden cardiac death [SCD]) from birth through age 40 years among 971 LQT1 (n = 549) and LQT2 (n = 422) patients from the International LQTS Registry. Risk factors for cardiac events included the LQT1 genotype (HR = 1.49, P = 0.003) and male gender (HR = 1.31, P = 0.04) in the 0-14 years age group; and the LQT2 genotype (HR = 1.67, P < 0.001) and female gender (HR = 2.58, P < 0.001) in the 15-40 years age group. Gender-genotype subset analysis showed enhanced risk among LQT1 males (HR = 1.93, P < 0.001) and LQT2 females (HR = 3.28, P < 0.001) in the 2 respective age groups. Beta-blocker therapy was associated with a significant risk-reduction in high-risk patients, including a 67% reduction (P = 0.02) in LQT1 males and a 71% reduction (P < 0.001) in LQT2 females. Life-threatening events (ACA/SCD) rarely occurred as a presenting symptom among beta-blocker-treated patients. However, high-risk patients who experienced syncope during beta-blocker therapy had a relatively high rate of subsequent ACA/SCD (>1 event per 100 patient-years).
Conclusions: The present findings suggest that beta-blocker therapy should be routinely administered to all high-risk LQT1 and LQT2 patients without contraindications as a first line measure, whereas primary defibrillator therapy should be recommended for those who experience syncope during medical therapy.
Figures



Comment in
-
Advice for management of the long-QT patient.J Cardiovasc Electrophysiol. 2010 Aug 1;21(8):902-4. doi: 10.1111/j.1540-8167.2010.01775.x. Epub 2010 Apr 23. J Cardiovasc Electrophysiol. 2010. PMID: 20455972 No abstract available.
References
-
- Goldenberg I, Moss AJ. Long QT syndrome. J Am Coll Cardiol. 2008;51:2291–2300. - PubMed
-
- Schwartz PJ, Priori SG, Spazzolini C, Moss AJ, Vincent GM, Napolitano C, Denjoy I, Guicheney P, Breithardt G, Keating MT, Towbin JA, Beggs AH, Brink P, Wilde AA, Toivonen L, Zareba W, Robinson JL, Timothy KW, Corfield V, Wattanasirichaigoon D, Corbett C, Haverkamp W, Schulze-Bahr E, Lehmann MH, Schwartz K, Coumel P, Bloise R. Genotype-phenotype correlation in the long-QT syndrome: gene-specific triggers for life-threatening arrhythmias. Circulation. 2001;103:89–95. - PubMed
-
- Wang Q, Curran ME, Splawski I, Burn TC, Millholland JM, VanRaay TJ, Shen J, Timothy KW, Vincent GM, de Jager T, Schwartz PJ, Toubin JA, Moss AJ, Atkinson DL, Landes GM, Connors TD, Keating MT. Positional cloning of a novel potassium channel gene: KVLQT1 mutations cause cardiac arrhythmias. Nat Genet. 1996;12:17–23. - PubMed
-
- Trudeau MC, Warmke JW, Ganetzky B, Robertson GA. HERG: a human inward rectifier in the voltage-gated potassium channel family. Science. 1995;269:92–95. - PubMed
-
- Schwartz PJ, Priori SG, Locati EH, Napolitano C, Cantù F, Towbin JA, Keating MT, Hammoude H, Brown AM, Chen LS. Long QT syndrome patients with mutations on the SCN5A and HERG genes have differential responses to Na+ channel blockade and to increases in heart rate. Implications for gene-specific therapy. Circulation. 1995;92:3381–3386. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
