

Regional lung aeration and ventilation during pressure support and biphasic positive airway pressure ventilation in experimental lung injury
- PMID: 20233399
- PMCID: PMC2887141
- DOI: 10.1186/cc8912
Regional lung aeration and ventilation during pressure support and biphasic positive airway pressure ventilation in experimental lung injury
Abstract
Introduction: There is an increasing interest in biphasic positive airway pressure with spontaneous breathing (BIPAP+SBmean), which is a combination of time-cycled controlled breaths at two levels of continuous positive airway pressure (BIPAP+SBcontrolled) and non-assisted spontaneous breathing (BIPAP+SBspont), in the early phase of acute lung injury (ALI). However, pressure support ventilation (PSV) remains the most commonly used mode of assisted ventilation. To date, the effects of BIPAP+SBmean and PSV on regional lung aeration and ventilation during ALI are only poorly defined.
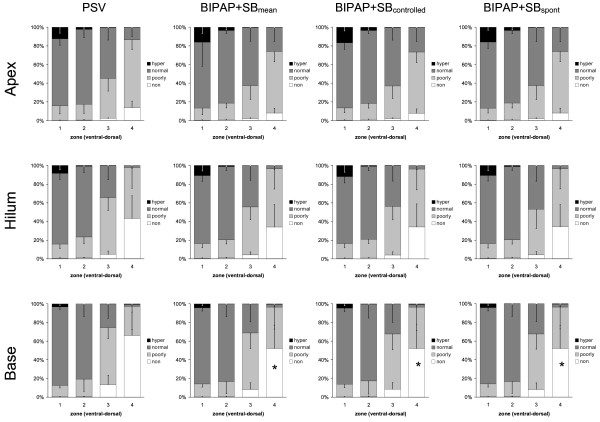
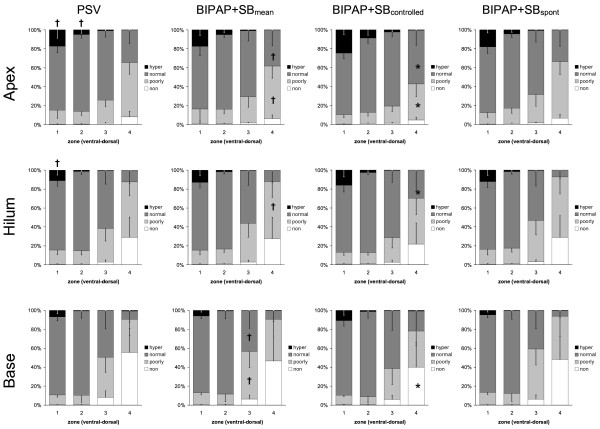
Methods: In 10 anesthetized juvenile pigs, ALI was induced by surfactant depletion. BIPAP+SBmean and PSV were performed in a random sequence (1 h each) at comparable mean airway pressures and minute volumes. Gas exchange, hemodynamics, and inspiratory effort were determined and dynamic computed tomography scans obtained. Aeration and ventilation were calculated in four zones along the ventral-dorsal axis at lung apex, hilum and base.
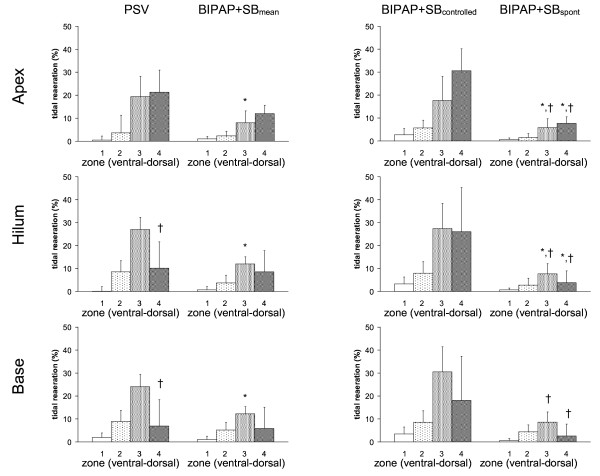
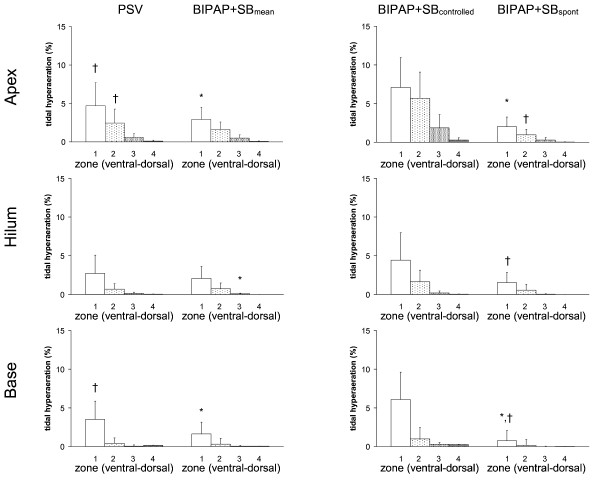
Results: Compared to PSV, BIPAP+SBmean resulted in: 1) lower mean tidal volume, comparable oxygenation and hemodynamics, and increased PaCO2 and inspiratory effort; 2) less nonaerated areas at end-expiration; 3) decreased tidal hyperaeration and re-aeration; 4) similar distributions of ventilation. During BIPAP+SBmean: i) BIPAP+SBspont had lower tidal volumes and higher rates than BIPAP+SBcontrolled; ii) BIPAP+SBspont and BIPAP+SBcontrolled had similar distributions of ventilation and aeration; iii) BIPAP+SBcontrolled resulted in increased tidal re-aeration and hyperareation, compared to PSV. BIPAP+SBspont showed an opposite pattern.
Conclusions: In this model of ALI, the reduction of tidal re-aeration and hyperaeration during BIPAP+SBmean compared to PSV is not due to decreased nonaerated areas at end-expiration or different distribution of ventilation, but to lower tidal volumes during BIPAP+SBspont. The ratio between spontaneous to controlled breaths seems to play a pivotal role in reducing tidal re-aeration and hyperaeration during BIPAP+SBmean.
Figures
References
-
- Putensen C, Zech S, Wrigge H, Zinserling J, Stuber F, von Spiegel T, Mutz N. Long-term effects of spontaneous breathing during ventilatory support in patients with acute lung injury. Am J Respir Crit Care Med. 2001;164:43–49. - PubMed
-
- Esteban A, Ferguson ND, Meade MO, Frutos-Vivar F, Apezteguia C, Brochard L, Raymondos K, Nin N, Hurtado J, Tomicic V, González M, Elizalde J, Nightingale P, Abroug F, Pelosi P, Arabi Y, Moreno R, Jibaja M, D'Empaire G, Sandi F, Matamis D, Montañez AM, Anzueto A. VENTILA Group. Evolution of mechanical ventilation in response to clinical research. Am J Respir Crit Care Med. 2008;177:170–177. doi: 10.1164/rccm.200706-893OC. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
