

A review of data needed to parameterize a dynamic model of measles in developing countries
- PMID: 20233414
- PMCID: PMC2848058
- DOI: 10.1186/1756-0500-3-75
A review of data needed to parameterize a dynamic model of measles in developing countries
Abstract
Background: Dynamic models of infection transmission can project future disease burden within a population. Few dynamic measles models have been developed for low-income countries, where measles disease burden is highest. Our objective was to review the literature on measles epidemiology in low-income countries, with a particular focus on data that are needed to parameterize dynamic models.
Methods: We included age-stratified case reporting and seroprevalence studies with fair to good sample sizes for mostly urban African and Indian populations. We emphasized studies conducted before widespread immunization. We summarized age-stratified attack rates and seroprevalence profiles across these populations. Using the study data, we fitted a "representative" seroprevalence profile for African and Indian settings. We also used a catalytic model to estimate the age-dependent force of infection for individual African and Indian studies where seroprevalence was surveyed. We used these data to quantify the effects of population density on the basic reproductive number R0.
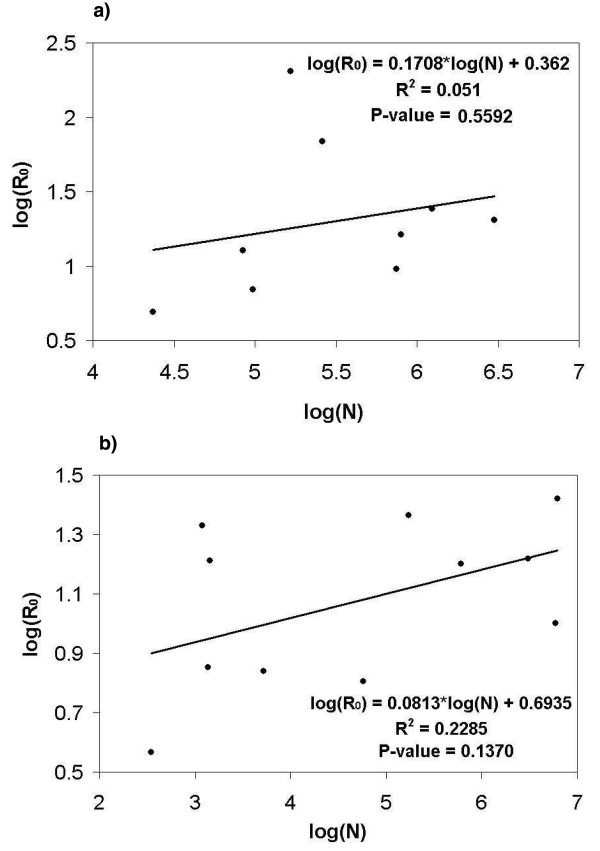
Results: The peak attack rate usually occurred at age 1 year in Africa, and 1 to 2 years in India, which is earlier than in developed countries before mass vaccination. Approximately 60% of children were seropositive for measles antibody by age 2 in Africa and India, according to the representative seroprevalence profiles. A statistically significant decline in the force of infection with age was found in 4 of 6 Indian seroprevalence studies, but not in 2 African studies. This implies that the classic threshold result describing the critical proportion immune (pc) required to eradicate an infectious disease, pc = 1-1/R0, may overestimate the required proportion immune to eradicate measles in some developing country populations. A possible, though not statistically significant, positive relation between population density and R0 for various Indian and African populations was also found. These populations also showed a similar pattern of waning of maternal antibodies. Attack rates in rural Indian populations show little dependence on vaccine coverage or population density compared to urban Indian populations. Estimated R0 values varied widely across populations which has further implications for measles elimination.
Conclusions: It is possible to develop a broadly informative dynamic model of measles transmission in low-income country settings based on existing literature, though it may be difficult to develop a model that is closely tailored to any given country. Greater efforts to collect data specific to low-income countries would aid in control efforts by allowing highly population-specific models to be developed.
Figures


Similar articles
-
The pre-vaccination regional epidemiological landscape of measles in Italy: contact patterns, effort needed for eradication, and comparison with other regions of Europe.Popul Health Metr. 2005 Feb 17;3(1):1. doi: 10.1186/1478-7954-3-1. Popul Health Metr. 2005. PMID: 15717921 Free PMC article.
-
Measles control in developing and developed countries: the case for a two-dose policy.Bull World Health Organ. 1993;71(1):93-103. Bull World Health Organ. 1993. PMID: 8440043 Free PMC article. Review.
-
Controlling measles using supplemental immunization activities: a mathematical model to inform optimal policy.Vaccine. 2015 Mar 3;33(10):1291-6. doi: 10.1016/j.vaccine.2014.11.050. Epub 2014 Dec 23. Vaccine. 2015. PMID: 25541214 Free PMC article.
-
The role of herd immunity in control of measles.Yale J Biol Med. 1982 May-Aug;55(3-4):351-60. Yale J Biol Med. 1982. PMID: 7180027 Free PMC article.
-
Scheduling of measles vaccination in low-income countries: projections of a dynamic model.Vaccine. 2009 Jun 24;27(31):4090-8. doi: 10.1016/j.vaccine.2009.04.079. Epub 2009 May 14. Vaccine. 2009. PMID: 19410622 Review.
Cited by
-
Effectiveness assessment of vaccination policy against measles epidemic in Japan using an age-time two-dimensional mathematical model.Environ Health Prev Med. 2012 Jan;17(1):34-43. doi: 10.1007/s12199-011-0217-y. Epub 2011 May 7. Environ Health Prev Med. 2012. PMID: 21553196 Free PMC article.
-
The role of research in viral disease eradication and elimination programs: lessons for malaria eradication.PLoS Med. 2011 Jan 25;8(1):e1000405. doi: 10.1371/journal.pmed.1000405. PLoS Med. 2011. PMID: 21311582 Free PMC article. Review.
-
Using models to shape measles control and elimination strategies in low- and middle-income countries: A review of recent applications.Vaccine. 2020 Jan 29;38(5):979-992. doi: 10.1016/j.vaccine.2019.11.020. Epub 2019 Nov 29. Vaccine. 2020. PMID: 31787412 Free PMC article. Review.
-
The potential impact of immunization campaign budget re-allocation on global eradication of paediatric infectious diseases.BMC Public Health. 2011 Sep 28;11:739. doi: 10.1186/1471-2458-11-739. BMC Public Health. 2011. PMID: 21955853 Free PMC article.
References
-
- Clements CJ, Strassburg M, Cutts FT, Torel C. The epidemiology of measles. World Health Stat Q. 1992;45:285–291. - PubMed
-
- Semba RD. Vitamin A and immunity to viral, bacterial and protozoan infections. P Nutr Soc. 1999;58:719–727. - PubMed
-
- Markowitz LE, Orenstein WA. Measles Vaccines. Pediatr Clin N Am. 1990;37:603–625. - PubMed
-
- World Health Organization. Measles, Fact sheet No. 286. http://www.who.int/mediacentre/factsheets/fs286/en/
LinkOut - more resources
Full Text Sources
