

Chemotherapy with 5-fluorouracil, cisplatin and streptozocin for neuroendocrine tumours
- PMID: 20234360
- PMCID: PMC2853102
- DOI: 10.1038/sj.bjc.6605618
Chemotherapy with 5-fluorouracil, cisplatin and streptozocin for neuroendocrine tumours
Abstract
Background: The role of chemotherapy for neuroendocrine tumours remains controversial and there is no standard regimen.
Method: We report the outcome for a consecutive series of chemonaive patients with metastatic or locally advanced neuroendocrine tumours treated with a combination of 5-fluorouracil (500 mg m(-2)), cisplatin (70 mg m(-2)) and streptozocin (1000 mg m(-2)) (FCiSt) administered three weekly for up to six cycles. Patients were assessed for radiological response, toxicity and survival.
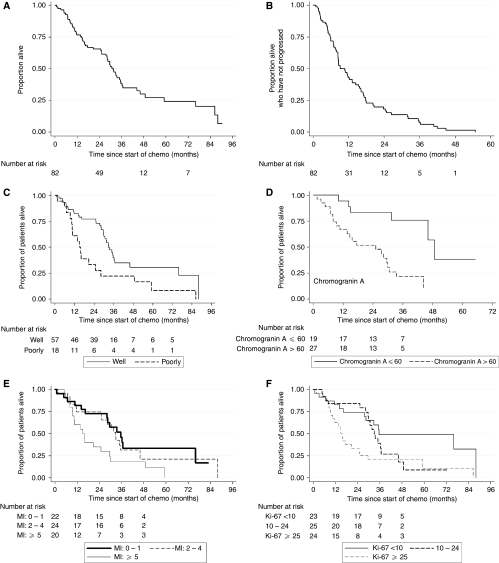
Results: In the 79 patients assessable for response, treatment with FCiSt was associated with an overall response rate of 33% (38% for pancreatic primary sites and 25% for non-pancreatic primary sites). Stable disease occurred in a further 51%, with progression in 16%. The median time to progression was 9.1 months and median overall survival was 31.5 months. The most common grade 3-4 toxicity was neutropaenia (28% patients) but grade 3-4 infection was rare (7%). The most frequent non-haematological grade 3-4 toxicity was nausea and vomiting (17%). Prognostic factors included Ki-67, mitotic index, grade and chromogranin A, whereas response to chemotherapy was predicted by mitotic index, grade and alpha-fetoprotein.
Conclusions: FCiSt is an effective regimen for neuroendocrine tumours with an acceptable toxicity profile. Grade and mitotic index are the best predictors of response.
Figures
References
-
- Ansell SM, Pitot HC, Burch PA, Kvols LK, Mahoney MR, Rubin J (2001) A phase II study of high-dose paclitaxel in patients with advanced neuroendocrine tumors. Cancer 91(8): 1543–1548 - PubMed
-
- Bukowski RM, Johnson KG, Peterson RF, Stephens RL, Rivkin SE, Neilan B, Costanzi JH (1987) A phase II trial of combination chemotherapy in patients with metastatic carcinoid tumors. A Southwest Oncology Group Study. Cancer 60(12): 2891–2895 - PubMed
-
- Cheng PN, Saltz LB (1999) Failure to confirm major objective antitumor activity for streptozocin and doxorubicin in the treatment of patients with advanced islet cell carcinoma. Cancer 86(6): 944–948 - PubMed
-
- Ekeblad S, Sundin A, Janson ET, Welin S, Granberg D, Kindmark H, Dunder K, Kozlovacki G, Orlefors H, Sigurd M, Oberg K, Eriksson B, Skogseid B (2007) Temozolomide as monotherapy is effective in treatment of advanced malignant neuroendocrine tumors. Clin Cancer Res 13(10): 2986–2991 - PubMed
-
- Engstrom PF, Lavin PT, Moertel CG, Folsch E, Douglass Jr HO (1984) Streptozocin plus fluorouracil versus doxorubicin therapy for metastatic carcinoid tumor. J Clin Oncol 2(11): 1255–1259 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
