

Twenty-first century laparoscopic hysterectomy: should we not leave the vaginal step out?
- PMID: 20234845
- PMCID: PMC2837251
- DOI: 10.1007/s10397-009-0481-7
Twenty-first century laparoscopic hysterectomy: should we not leave the vaginal step out?
Abstract
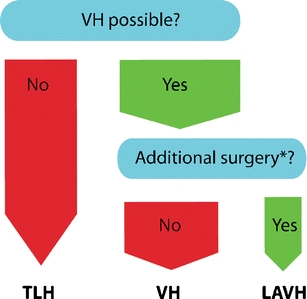
The objective of this study was to compare surgical outcomes for laparoscopically assisted vaginal hysterectomy (LAVH) with total laparoscopic hysterectomy (TLH) in three teaching hospitals in the Netherlands. This study is a multicenter cohort retrospective analysis of consecutive cases (Canadian Task Force classification II-2). One hundred and four women underwent a laparoscopic hysterectomy between March 1995 and March 2005 at one of three teaching hospitals. This included 37 women who underwent LAVH and 67 who underwent TLH. Blood loss, operating time, and intraoperative complications such as bladder or ureteric injury as well as conversion to an open procedure were recorded. In the TLH group, average age was statistically significant lower, as well as the mean parity, whereas estimated uterus size was statistically significant larger, compared to the LAVH group. Main indication in both groups was dysfunctional uterine bleeding. In the TLH group, mean blood loss (173 mL) was significant lower compared to the LAVH group (457 mL), whereas length of surgery, uterus weight, and complication rates were comparable between the two groups. The method of choice at the start of the study period was LAVH, and by the end of the study period, it had been superceded by TLH. LAVH should not be regarded as the novice's laparoscopic hysterectomy. Moreover, with regard blood loss, TLH shows advantages above LAVH. This might be due to the influence of the altered anatomy in the vaginal stage of the LAVH procedure. Therefore, when a vaginal hysterectomy is contraindicated, TLH is the procedure of choice. LAVH remains indicated in case of vaginal hysterectomy with accompanying adnexal surgery.
Figures
References
LinkOut - more resources
Full Text Sources