

Effects of duration of glucocorticoid therapy on relapse rate in antineutrophil cytoplasmic antibody-associated vasculitis: A meta-analysis
- PMID: 20235186
- PMCID: PMC2946200
- DOI: 10.1002/acr.20176
Effects of duration of glucocorticoid therapy on relapse rate in antineutrophil cytoplasmic antibody-associated vasculitis: A meta-analysis
Abstract
Objective: Disease relapses are common for patients with antineutrophil cytoplasmic antibody-associated vasculitis (AAV). The role of low-dose glucocorticoids (GC) in relapse prevention is controversial. We undertook a systematic review and meta-analysis to determine if GC target doses influence relapses of AAV.
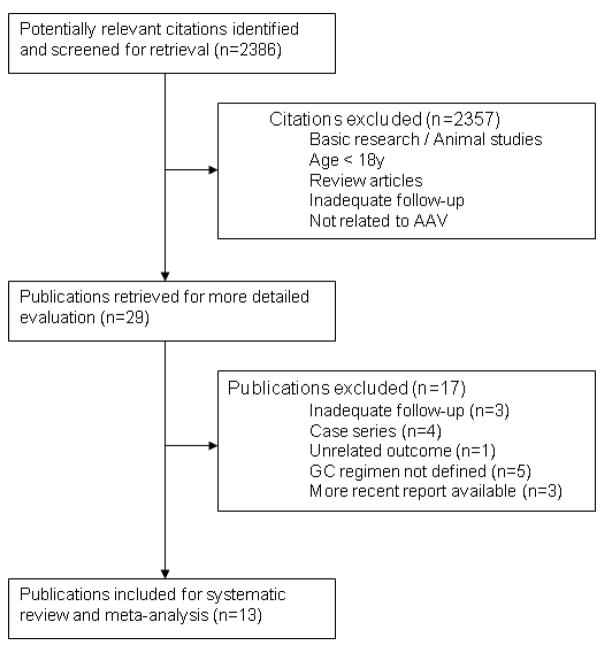
Methods: Medline, EMBase, and Cochrane databases were searched for observational studies and randomized controlled trials of treatment of AAV that included a predefined GC treatment plan. The association of GC target dose with the proportion of relapses in studies was assessed using meta-regression and multilevel generalized linear modeling.
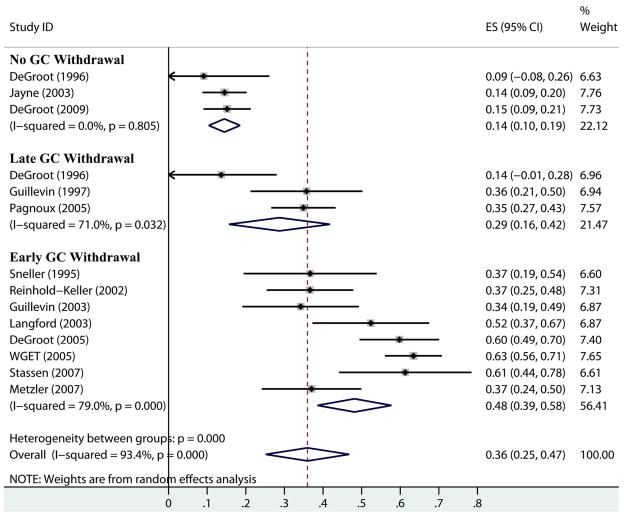
Results: Thirteen studies (983 patients) were identified for inclusion. There were no studies directly comparing GC regimens. We classified 288 patients as having a nonzero GC target dose by study end and 695 patients as having a zero GC target dose by study end. The pooled proportion of patients with a relapse was 36% (95% confidence interval [95% CI] 25-47%). GC regimen was the most significant variable explaining the variability between the proportions of patients with relapses. The proportion of patients with a relapse was 14% (95% CI 10-19%) in nonzero GC target dose studies and 43% (95% CI 33-52%) in zero GC target dose studies. Differences other than GC regimens exist between studies that complicate the comparability of trials and isolation of the variability in relapses due to GC target alone.
Conclusion: Studies with longer courses of GC in AAV are associated with fewer relapses. These results have implications for study design and outcome assessment in clinical trials of AAV.
Figures
References
-
- Frohnert PF, Sheps SG. Long-term folow-up study of periarteritis nodosa. Am J Med. 1967;43:8–11. - PubMed
-
- Fauci AS, Wolff SM, Johnson JS. Effect of cyclophosphamide upon the immune response in Wegener’s granulomatosis. N Engl J Med. 1971;285(27):1493–6. - PubMed
-
- Novack SN, Pearson CM. Cyclophosphamide therapy in Wegener’s granulomatosis. N Engl J Med. 1971;284(17):938–42. - PubMed
-
- Leib ES, Restivo C, Paulus HE. Immunosuppressive and corticosteroid therapy of polyarteritis nodosa. Am J Med. 1979;67:941–5. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
