

Themes of liver transplantation
- PMID: 20235333
- PMCID: PMC4507423
- DOI: 10.1002/hep.23595
Themes of liver transplantation
Abstract
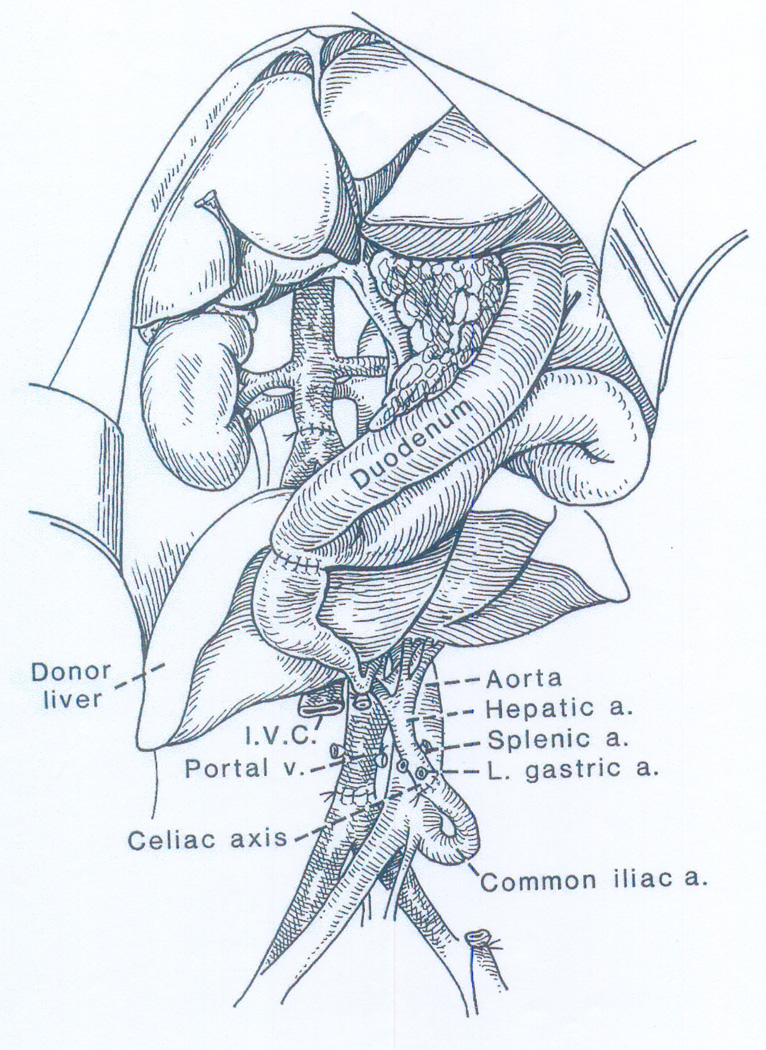
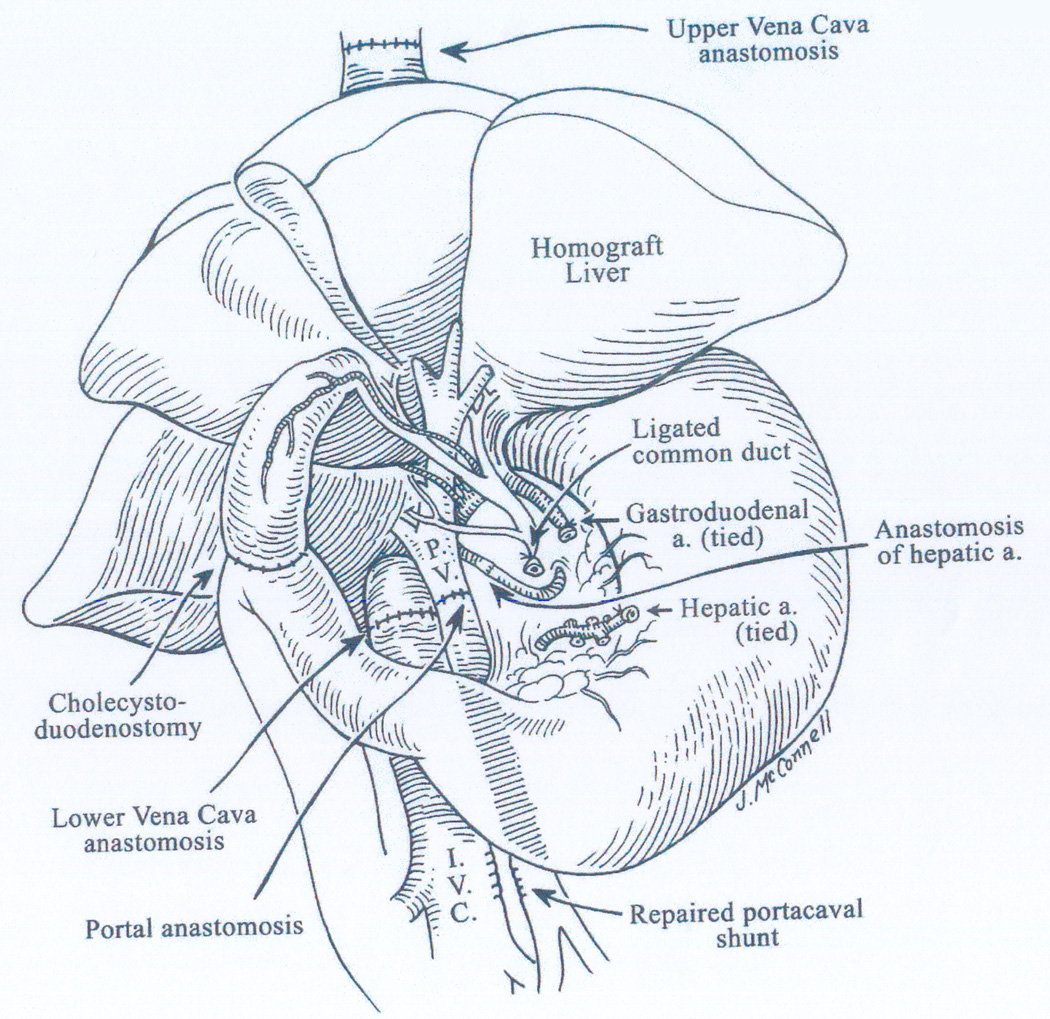
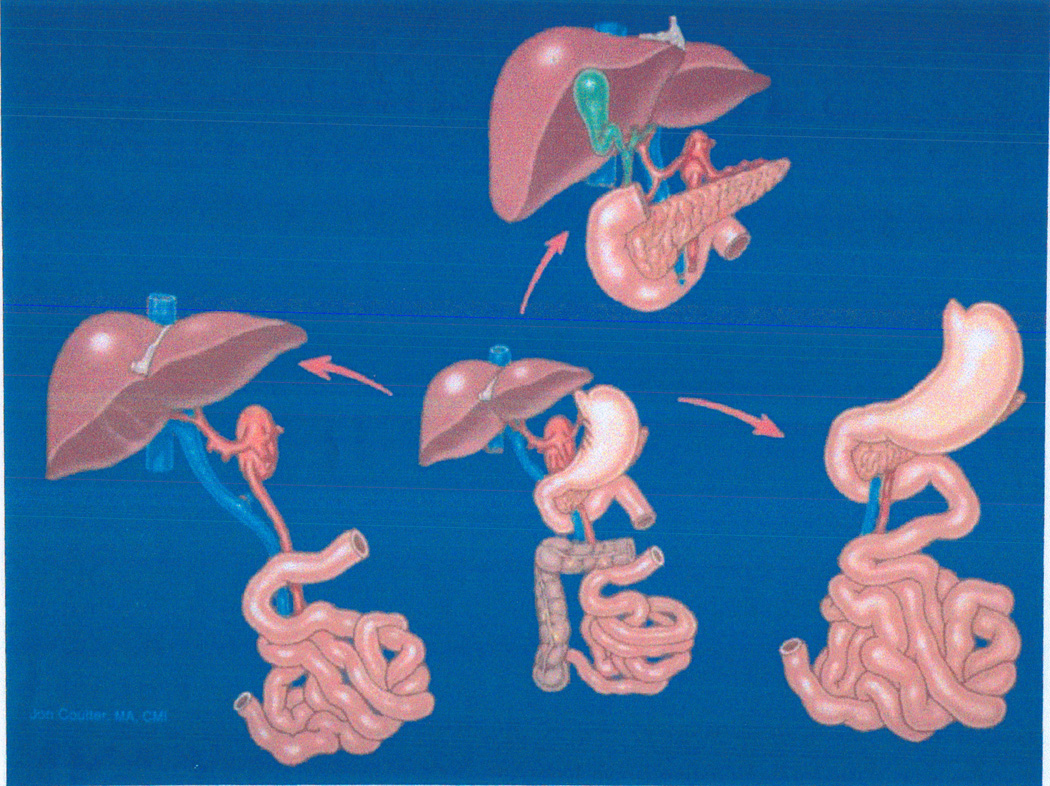
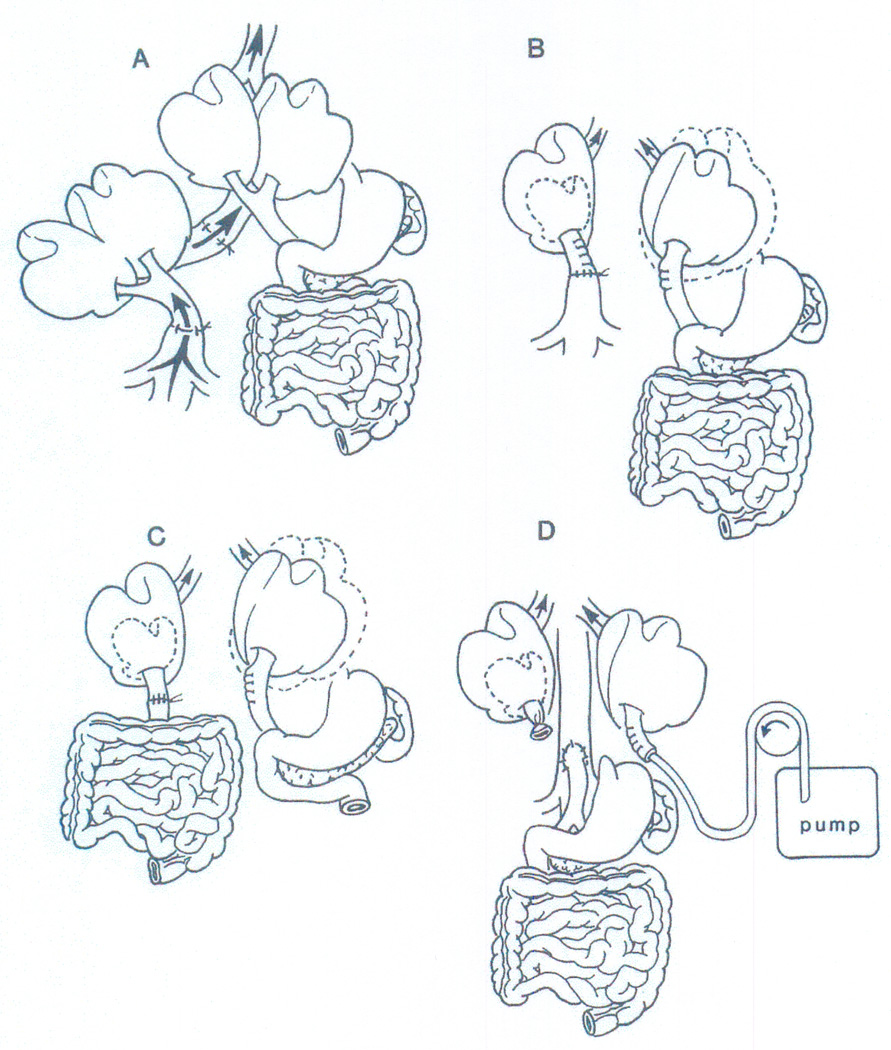
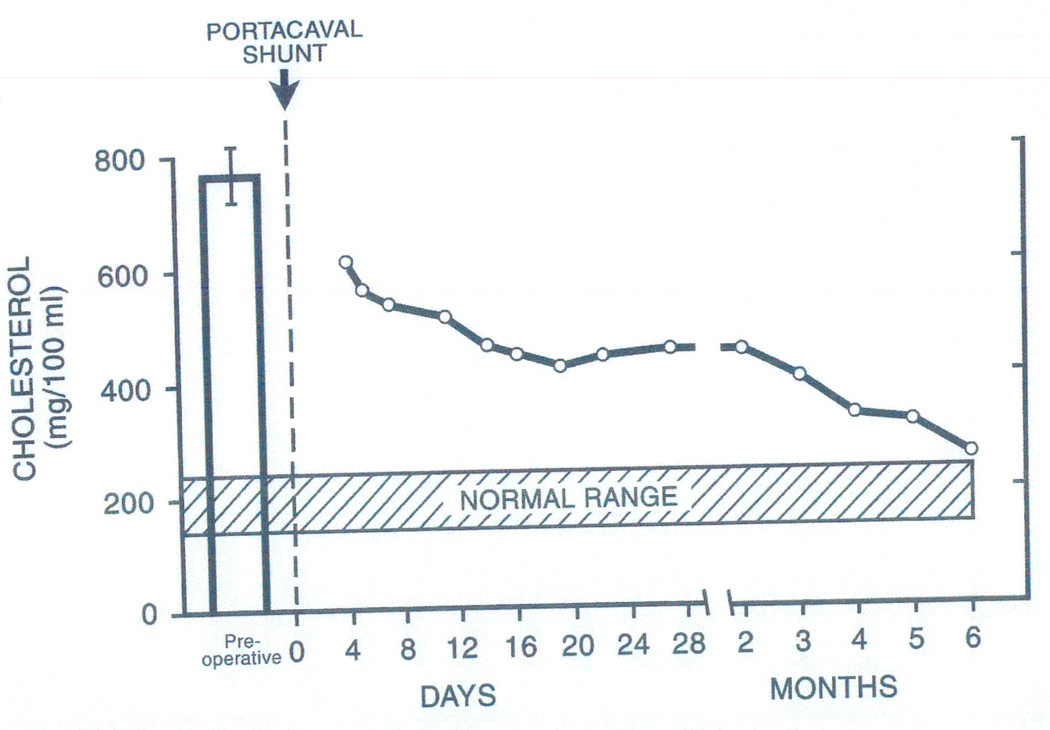
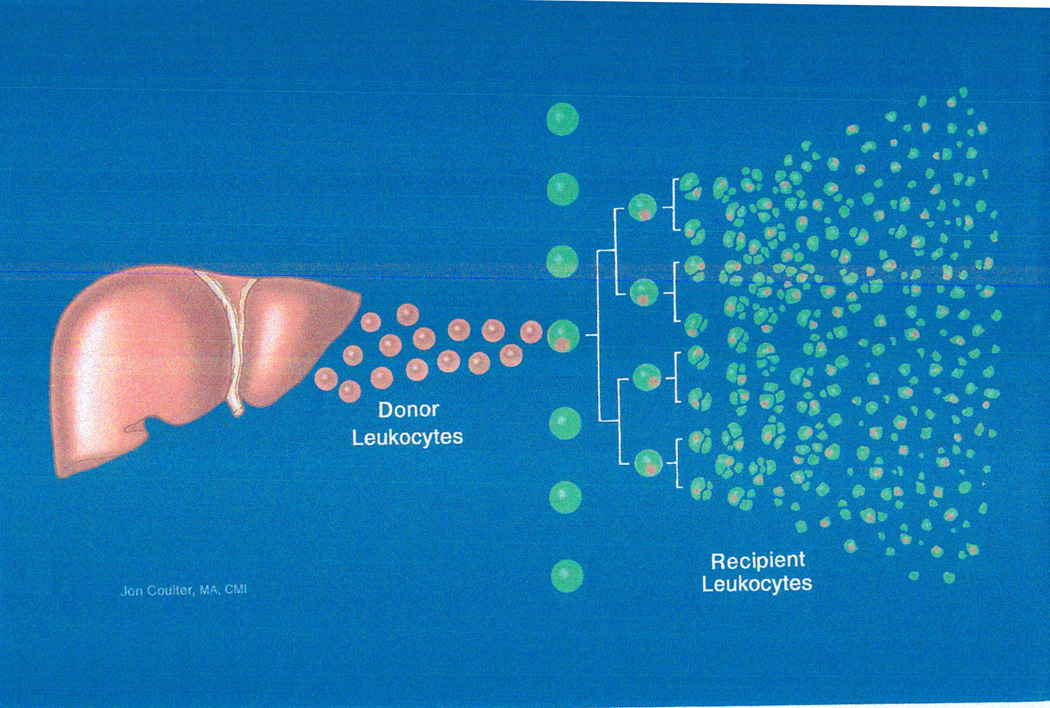
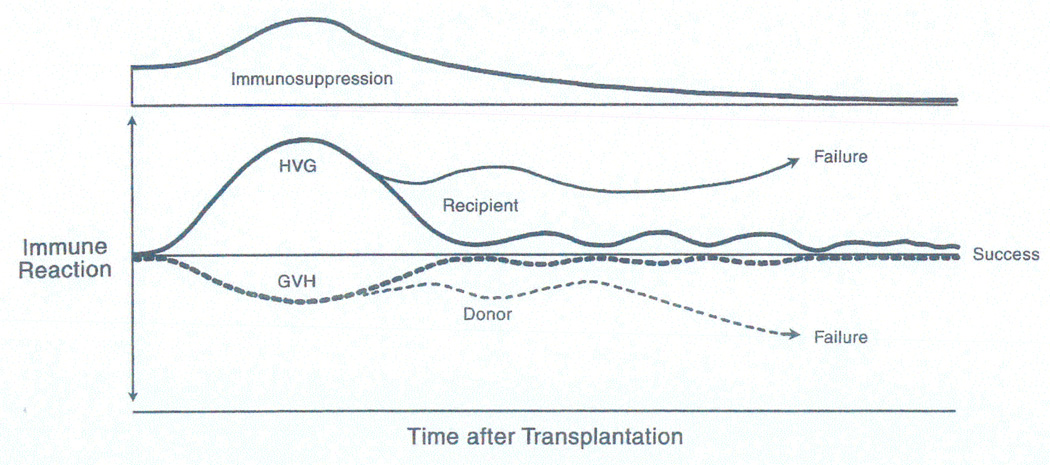
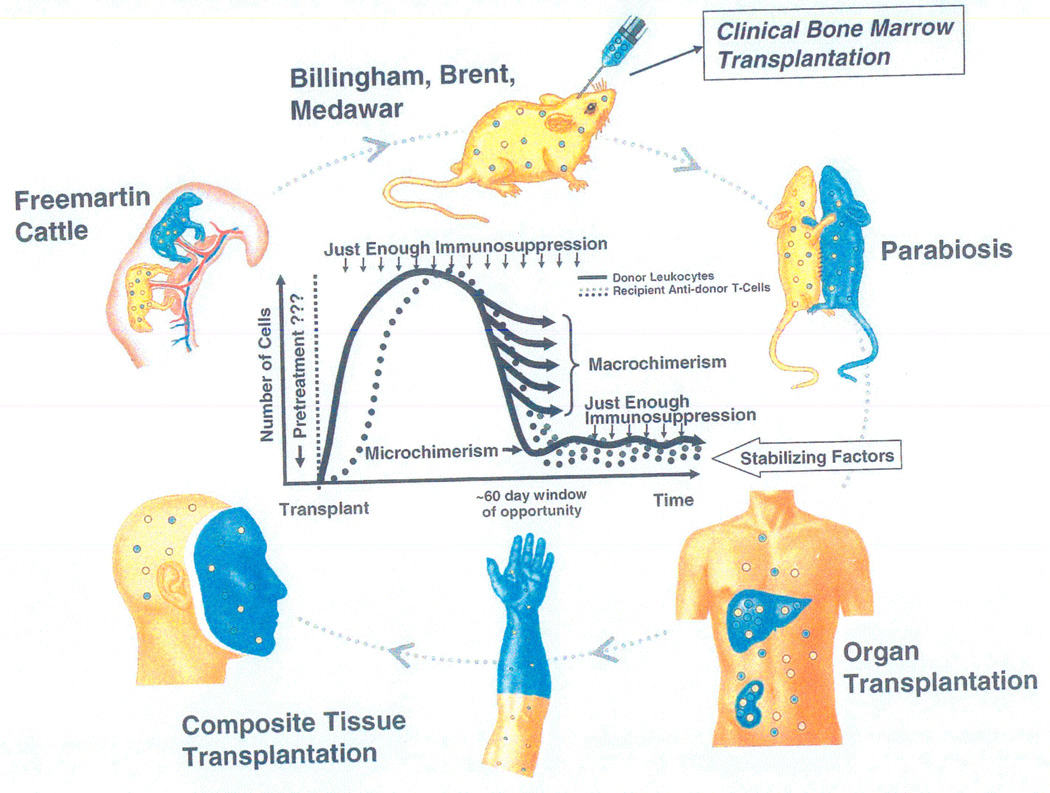
Liver transplantation was the product of five interlocking themes. These began in 1958-1959 with canine studies of then theoretical hepatotrophic molecules in portal venous blood (Theme I) and with the contemporaneous parallel development of liver and multivisceral transplant models (Theme II). Further Theme I investigations showed that insulin was the principal, although not the only, portal hepatotrophic factor. In addition to resolving long-standing controversies about the pathophysiology of portacaval shunt, the hepatotrophic studies blazed new trails in the regulation of liver size, function, and regeneration. They also targeted inborn metabolic errors (e.g., familial hyperlipoproteinemia) whose palliation by portal diversion presaged definitive correction with liver replacement. Clinical use of the Theme II transplant models depended on multiple drug immunosuppression (Theme III, Immunology), guided by an empirical algorithm of pattern recognition and therapeutic response. Successful liver replacement was first accomplished in 1967 with azathioprine, prednisone, and antilymphoid globulin. With this regimen, the world's longest surviving liver recipient is now 40 years postoperative. Incremental improvements in survival outcome occurred (Theme IV) when azathioprine was replaced by cyclosporine (1979), which was replaced in turn by tacrolimus (1989). However, the biologic meaning of alloengraftment remained enigmatic until multilineage donor leukocyte microchimerism was discovered in 1992 in long-surviving organ recipients. Seminal mechanisms were then identified (clonal exhaustion-deletion and immune ignorance) that linked organ engraftment and the acquired tolerance of bone marrow transplantation and eventually clarified the relationship of transplantation immunology to the immunology of infections, neoplasms, and autoimmune disorders. With this insight, better strategies of immunosuppression have evolved. As liver and other kinds of organ transplantation became accepted as healthcare standards, the ethical, legal, equity, and the other humanism issues of Theme V have been resolved less conclusively than the medical-scientific problems of Themes I-IV.
Figures
References
-
- Welch CS. A note on transplantation of the whole liver in dogs. Transplant Bull. 1955;2:54–55.
-
- Moore FD, Smith LL, Burnap TK, Dallenbach FD, Dammin GJ, Gruber UF, Shoemaker WC, Steenburg RW, Ball MR, Belko JS. One-stage homotransplantation of the liver following total hepatectomy in dogs. Transplant Bull. 1959;6:103–110. - PubMed
Publication types
MeSH terms
Personal name as subject
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials